

Aquaporin 4 IgG serostatus and outcome in recurrent longitudinally extensive transverse myelitis
- PMID: 24248262
- PMCID: PMC3934000
- DOI: 10.1001/jamaneurol.2013.5055
Aquaporin 4 IgG serostatus and outcome in recurrent longitudinally extensive transverse myelitis
Abstract
Importance: Studies focused on recurrent longitudinally extensive transverse myelitis (rLETM) are lacking.
Objectives: To determine the aquaporin 4 (AQP4) IgG detection rate using recombinant human APQ4-based assays in sequential serum specimens collected from patients with rLETM categorized as negative by first-generation tissue-based indirect immunofluorescence (IIF) assay and to define the clinical characteristics and motor disability outcomes in AQP4-IgG-positive rLETM.
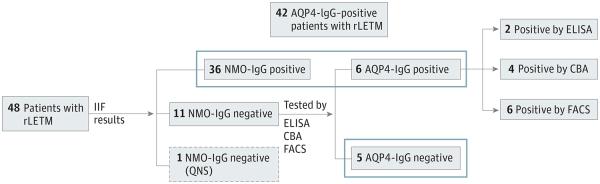
Design, setting, and participants: A search of the Mayo Clinic computerized central diagnostic index (October 1, 2005, through November 30, 2011), cross-linked with the Neuroimmunology Laboratory database, identified 48 patients with rLETM, of whom 36 (75%) were positive and 12 (25%) negative for neuromyelitis optica (NMO) IgG (per IIF of serial serum specimens). Stored serum specimens from "seronegative" patients were retested with recombinant human AQP4-based assays, including enzyme-linked immunosorbent, transfected cell-based, and fluorescence-activated cell-sorting assays. Control patients included 140 AQP4-IgG-positive patients with NMO, of whom a subgroup of 20 initially presented with 2 attacks of transverse myelitis (rLETM-onset NMO).
Main outcomes and measures: AQP4-IgG serostatus, clinical characteristics, and Expanded Disability Status Scale score.
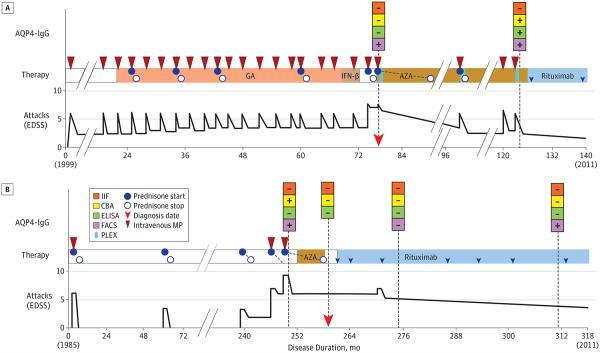
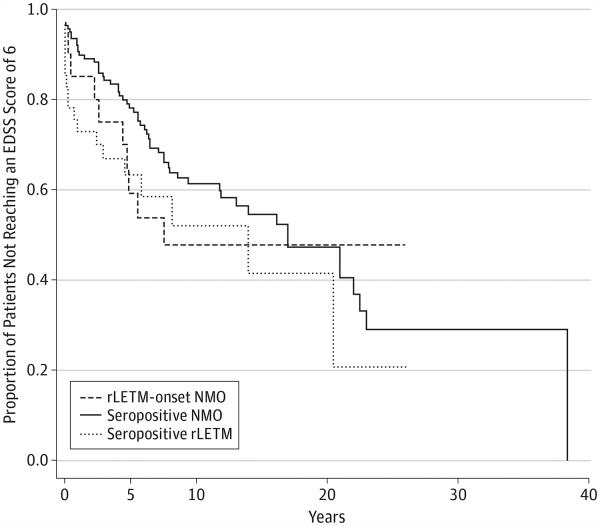
Results: Six patients with negative IIF results were reclassified as AQP4-IgG positive, yielding an overall AQP4-IgG seropositivity rate of 89%. Fluorescence-activated cell-sorting, cell-based, and enzyme-linked immunosorbent assays improved the detection rate to 89%, 85%, and 81%, respectively. The female to male ratio was 2:3 for AQP4-IgG-negative rLETM and 5:1 for AQP4-IgG-positive patients. The AQP4-IgG-positive patients with rLETM or rLETM-onset NMO were similar in age at onset, sex ratio, attack severity, relapse rate, and motor disability. From Kaplan-Meier analyses, 36% of AQP4-IgG-positive patients with rLETM are anticipated to need a cane to walk within 5 years after onset. For patients with rLETM-onset NMO, the median time from onset to first optic neuritis attack (54 months) was similar to the median disease duration for AQP4-IgG-positive patients with rLETM (59 months). The median number of attacks was 3 for AQP4-IgG-positive patients with rLETM (range, 2-22), and the first optic neuritis attack for those with rLETM-onset NMO followed a median of 3 myelitis attacks (range, 2-19). Immunosuppressant therapy reduced the relapse rate in both AQP4-IgG-positive and AQP4-IgG-negative patients with rLETM.
Conclusions and relevance: Recombinant antigen-based assays significantly increase AQP4-IgG detection in patients with rLETM, and AQP4-IgG-negative adults with rLETM are rare. Evolution to NMO can be anticipated in AQP4-IgG-positive patients. Early initiation of immunotherapy may result in a more favorable motor outcome.
Figures
References
-
- Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. The spectrum of neuromyelitis optica. Lancet Neurol. 2007;6(9):805–815. - PubMed
-
- Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica. Neurology. 2006;66(10):1485–1489. - PubMed
-
- Weinshenker BG, Wingerchuk DM, Vukusic S, et al. Neuromyelitis optica IgG predicts relapse after longitudinally extensive transverse myelitis. Ann Neurol. 2006;59(3):566–569. - PubMed
-
- Pittock SJ, Lucchinetti CF. Inflammatory transversemyelitis: evolving concepts. Curr Opin Neurol. 2006;19(4):362–368. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
