

Worldwide trends in incidence rates for oral cavity and oropharyngeal cancers
- PMID: 24248688
- PMCID: PMC3865341
- DOI: 10.1200/JCO.2013.50.3870
Worldwide trends in incidence rates for oral cavity and oropharyngeal cancers
Abstract
Purpose: Human papillomavirus (HPV) has been identified as the cause of the increasing oropharyngeal cancer (OPC) incidence in some countries. To investigate whether this represents a global phenomenon, we evaluated incidence trends for OPCs and oral cavity cancers (OCCs) in 23 countries across four continents.
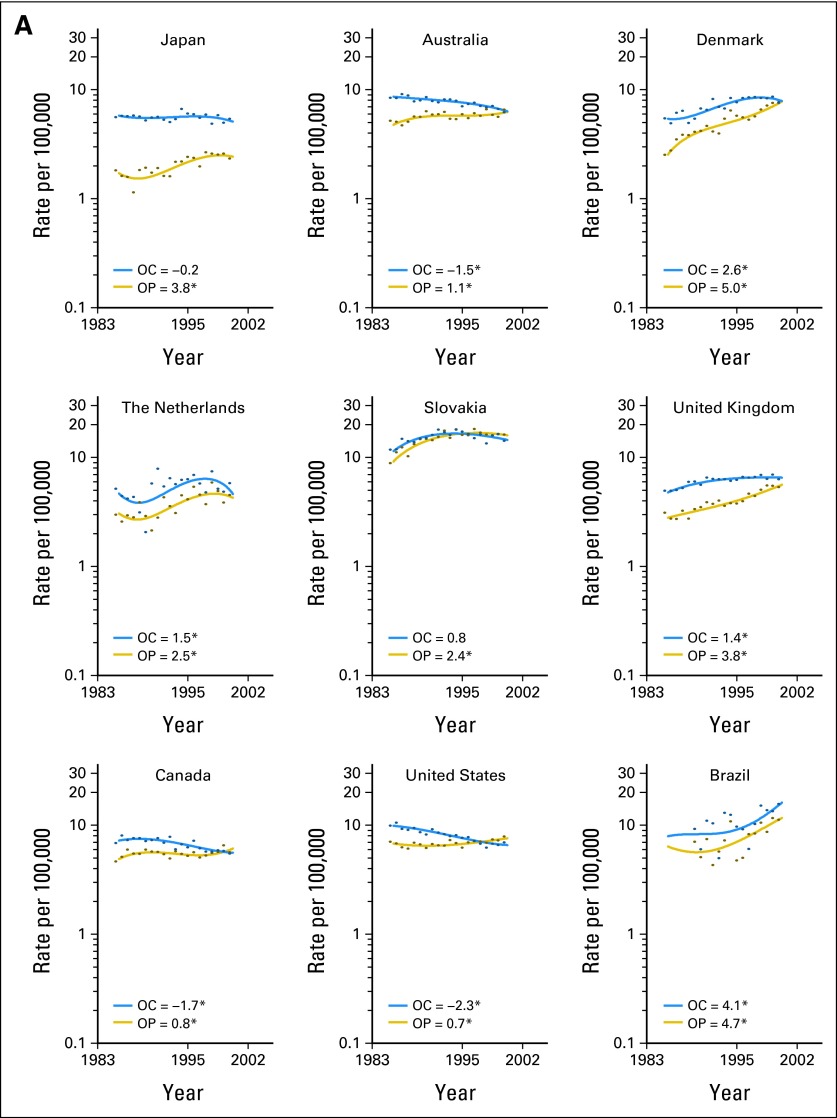
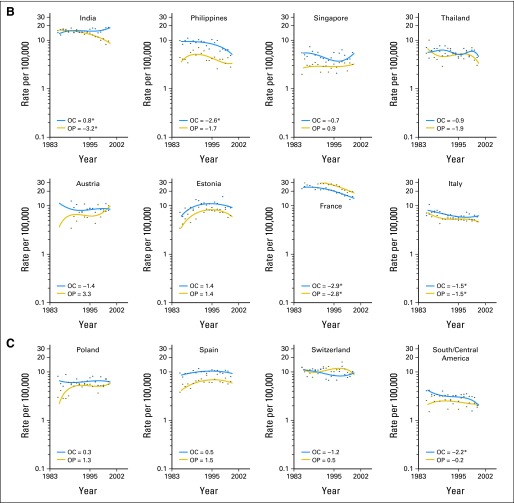
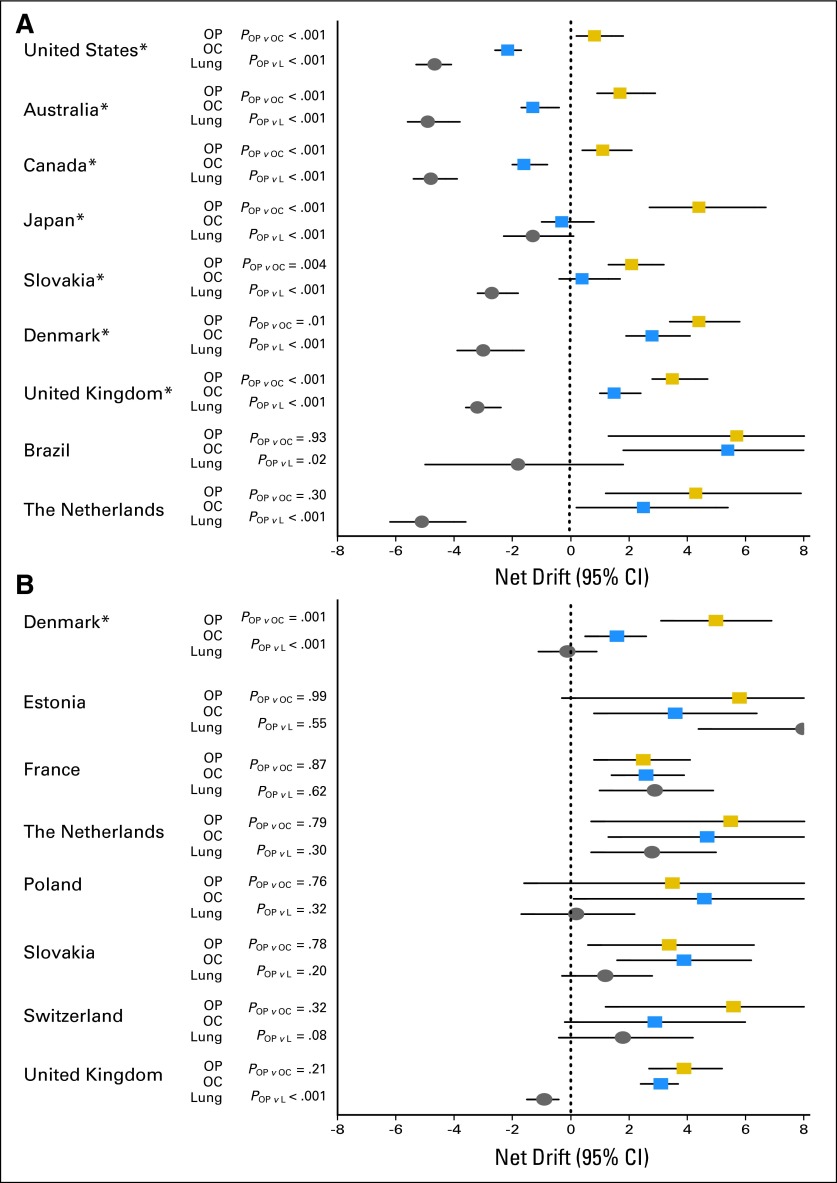
Methods: We used data from the Cancer Incidence in Five Continents database Volumes VI to IX (years 1983 to 2002). Using age-period-cohort modeling, incidence trends for OPCs were compared with those of OCCs and lung cancers to delineate the potential role of HPV vis-à-vis smoking on incidence trends. Analyses were country specific and sex specific.
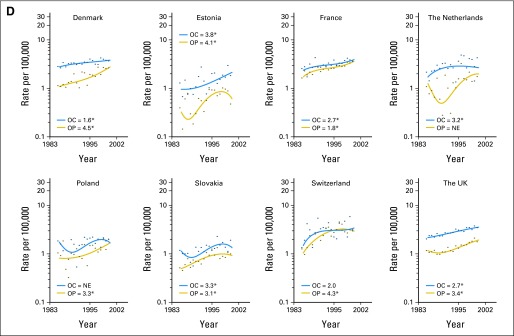
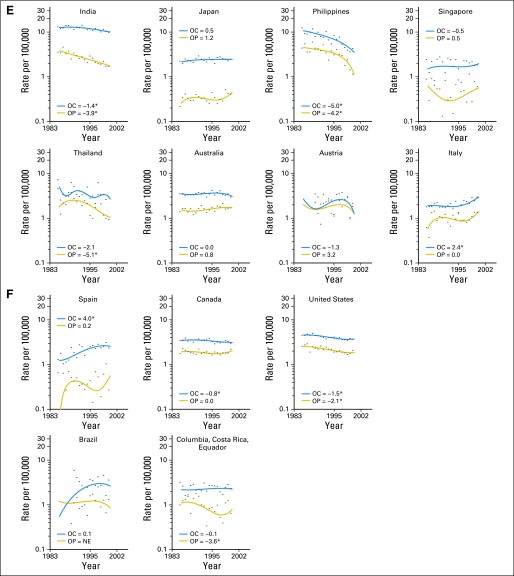
Results: OPC incidence significantly increased during 1983 to 2002 predominantly in economically developed countries. Among men, OPC incidence significantly increased in the United States, Australia, Canada, Japan, and Slovakia, despite nonsignificant or significantly decreasing incidence of OCCs. In contrast, among women, in all countries with increasing OPC incidence (Denmark, Estonia, France, the Netherlands, Poland, Slovakia, Switzerland, and United Kingdom), there was a concomitant increase in incidence of OCCs. Although increasing OPC incidence among men was accompanied by decreasing lung cancer incidence, increasing incidence among women was generally accompanied by increasing lung cancer incidence. The magnitude of increase in OPC incidence among men was significantly higher at younger ages (< 60 years) than older ages in the United States, Australia, Canada, Slovakia, Denmark, and United Kingdom.
Conclusion: OPC incidence significantly increased during 1983 to 2002 predominantly in developed countries and at younger ages. These results underscore a potential role for HPV infection on increasing OPC incidence, particularly among men.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–2917. - PubMed
-
- Blot WJ, McLaughlin JK, Winn DM, et al. Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res. 1988;48:3282–3287. - PubMed
-
- Hashibe M, Brennan P, Benhamou S, et al. Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: Pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. J Natl Cancer Inst. 2007;99:777–789. - PubMed
-
- D'Souza G, Kreimer AR, Viscidi R, et al. Case-control study of human papillomavirus and oropharyngeal cancer. N Engl J Med. 2007;356:1944–1956. - PubMed
-
- Gillison ML, Koch WM, Capone RB, et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst. 2000;92:709–720. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
