

Beyond the androgen receptor: new approaches to treating metastatic prostate cancer. Report of the 2013 Prouts Neck Prostate Cancer Meeting
- PMID: 24249419
- PMCID: PMC4253084
- DOI: 10.1002/pros.22753
Beyond the androgen receptor: new approaches to treating metastatic prostate cancer. Report of the 2013 Prouts Neck Prostate Cancer Meeting
Abstract
Introduction: The Prouts Neck Meetings on Prostate Cancer began in 1985 through the efforts of the Organ Systems Branch of the National Cancer Institute to stimulate new research and focused around specific questions in prostate tumorigenesis and therapy.
Methods: These meetings were think tanks, composed of around 75 individuals, and divided equally between young investigators and senior investigators. Over the years, many new concepts related to prostate cancer resulted from these meetings and the prostate cancer community has sorely missed them since the last one in 2007.
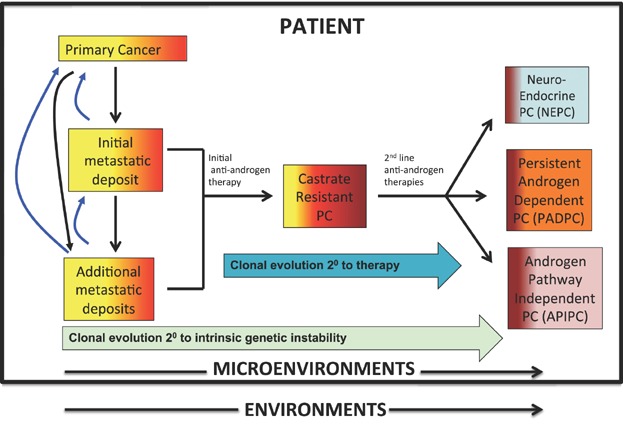
Results: We report here the first of a new series of meetings. The 2013 meeting focused on defining how the field of treatment for metastatic prostate cancer needs to evolve to impact survival and was entitled: "Beyond AR: New Approaches to Treating Metastatic Prostate Cancer." As castrate resistant prostate cancers escape second generation anti-androgen agents, three phenotypes/genotypes of CRPC appear to be increasing in prevalence and remain resistant to treatment: NeuroEndocrine Prostate Cancer, Persistent AR-Dependent Prostate Cancer, and Androgen Receptor Pathway Independent Prostate Cancer.
Discussion: It is clear that new treatment paradigms need to be developed for this diverse group of diseases. The Prouts Neck 2013 Meeting on Prostate Cancer helped to frame the current state of the field and jumpstart ideas for new avenues of treatment.
Keywords: diagnostics; metastases; therapeutics; treatment resistance; tumor microenvironment.
© 2013 Wiley Periodicals, Inc.
Figures
References
-
- Soloway MS, deKernion JB, Gibbons RP, Johnson DE, Loening SA, Pontes JE, Prout GR, Jr, Schmidt JD, Scott WW, Chu TM, Gaeta JF, Slack NH, Murphy GP. Comparison of estramustine phosphate and vincristine alone or in combination for patients with advanced, hormone refractory, previously irradiated carcinoma of the prostate. J Urol. 1981;125(5):664–667. - PubMed
-
- Tannock IF, Osoba D, Stockler MR, Ernst DS, Neville AJ, Moore MJ, Armitage GR, Wilson JJ, Venner PM, Coppin CM, Murphy KC. Chemotherapy with mitoxantrone plus prednisone or prednisone alone for symptomatic hormone-resistant prostate cancer: A Canadian randomized trial with palliative end points. J Clin Oncol. 1996;14(6):1756–1764. - PubMed
-
- Saad F, Gleason DM, Murray R, Tchekmedyian S, Venner P, Lacombe L, Chin JL, Vinholes JJ, Goas JA, Chen B Zoledronic Acid Prostate Cancer Study Group. A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma. J Natl Cancer Inst. 2002;94(19):1458–1468. - PubMed
-
- Tannock IF, de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, Oudard S, Théodore C, James ND, Turesson I, Rosenthal MA, Eisenberger MA TAX 327 Investigators. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351(15):1502–1512. - PubMed
-
- Kantoff PW, Higano CS, Shore ND, Berger ER, Small EJ, Penson DF, Redfern CH, Ferrari AC, Dreicer R, Sims RB, Xu Y, Frohlich MW, Schellhammer PF IMPACT Study Investigators. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363(5):411–422. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
