

Myocardial damage detected by late gadolinium enhancement cardiovascular magnetic resonance is associated with subsequent hospitalization for heart failure
- PMID: 24249712
- PMCID: PMC3886781
- DOI: 10.1161/JAHA.113.000416
Myocardial damage detected by late gadolinium enhancement cardiovascular magnetic resonance is associated with subsequent hospitalization for heart failure
Abstract
Background: Hospitalization for heart failure (HHF) is among the most important problems confronting medicine. Late gadolinium enhancement (LGE) cardiovascular magnetic resonance (CMR) robustly identifies intrinsic myocardial damage. LGE may indicate inherent vulnerability to HHF, regardless of etiology, across the spectrum of heart failure stage or left ventricular ejection fraction (LVEF).
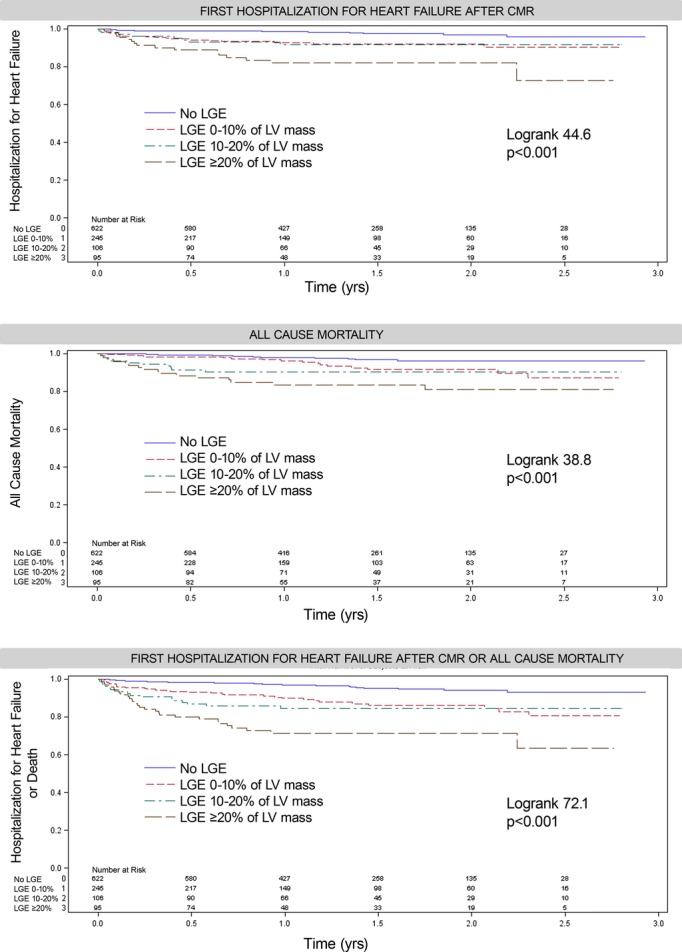
Methods and results: We enrolled 1068 consecutive patients referred for CMR where 448 (42%) exhibited LGE. After a median of 1.4 years (Q1 to Q3: 0.9 to 2.0 years), 57 HHF events occurred, 15 deaths followed HHF, and 43 deaths occurred without antecedent HHF (58 total deaths). Using multivariable Cox regression adjusting for LVEF, heart failure stage, and other covariates, LGE was associated with first HHF after CMR (HR: 2.70, 95% CI: 1.32 to 5.50), death (HR: 2.13, 95% CI: 1.08 to 4.21), or either death or HHF (HR: 2.52, 95% CI: 1.49 to 4.25). Quantifying LGE extent yielded similar results; more LGE equated higher risks. LGE improved model discrimination (IDI: 0.016, 95% CI: 0.005 to 0.028, P=0.002) and reclassification of individuals at risk (continuous NRI: 0.40, 95% CI: 0.05 to 0.70, P=0.024). Adjustment for competing risks of death that shares common risk factors with HHF strengthened the LGE and HHF association (HR: 4.85, 95% CI: 1.40 to 16.9).
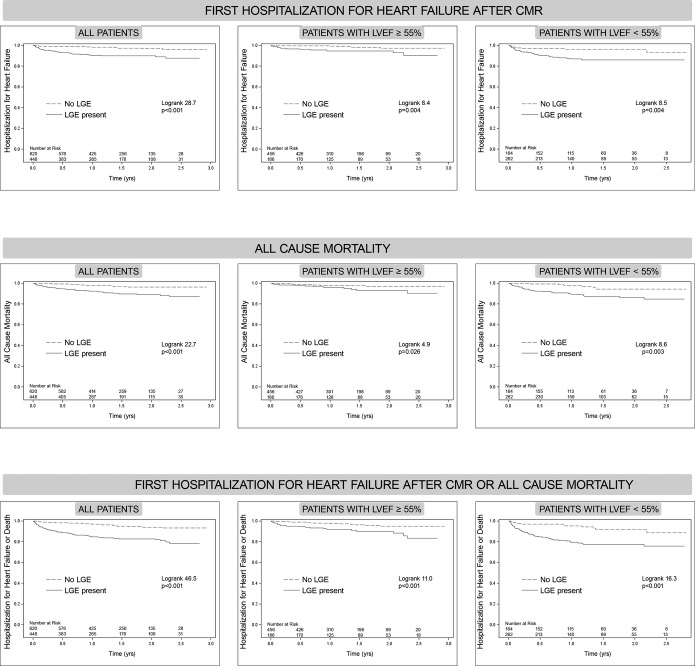
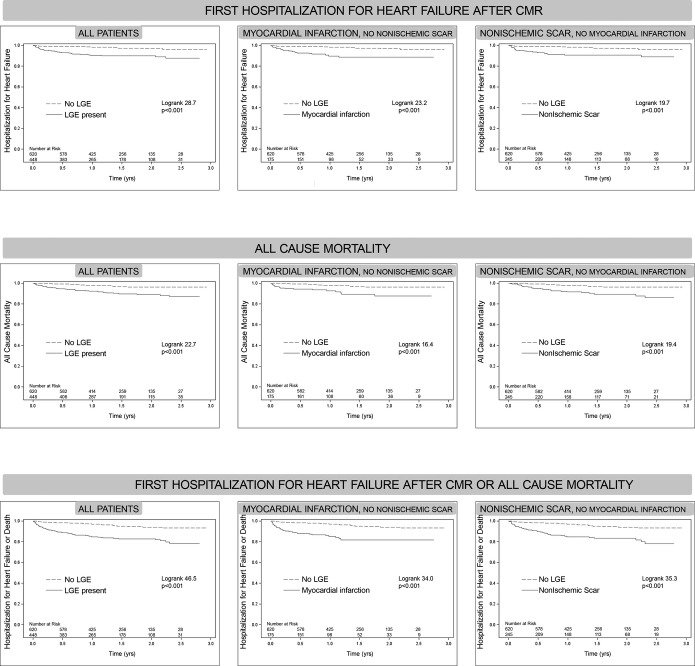
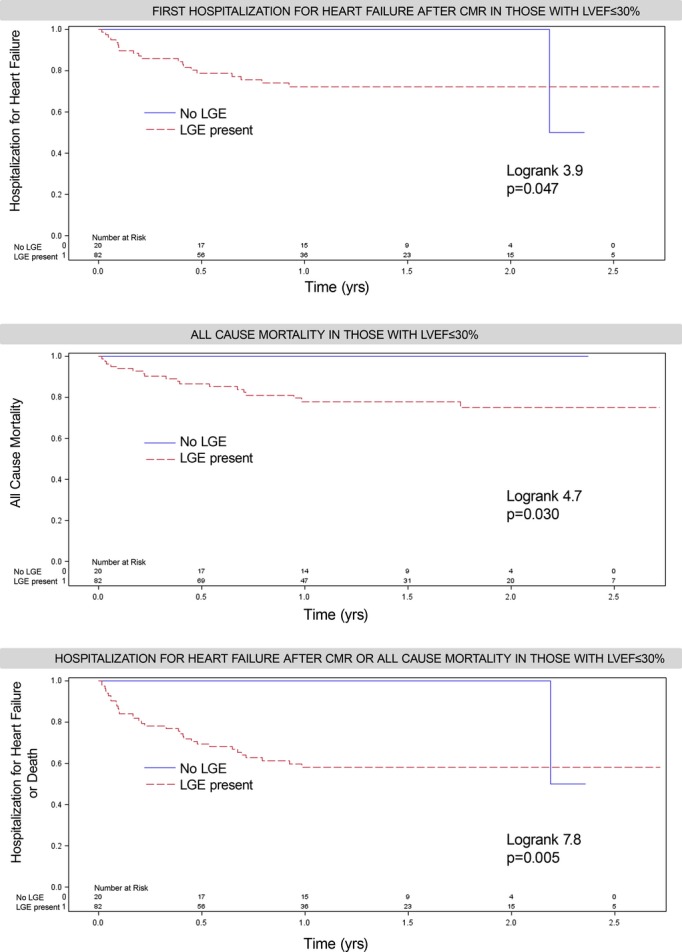
Conclusions: The presence and extent of LGE is associated with vulnerability for HHF, including higher risks of HHF across the spectrum of heart failure stage and LVEF. Even when LVEF is severely decreased, those without LGE appear to fare reasonably well. LGE may enhance risk stratification for HHF and may enhance both clinical and research efforts to reduce HHF through targeted treatment.
Keywords: late gadolinium enhancement; magnetic resonance imaging; myocardial delayed enhancement; myocardial fibrosis; myocardial infarction.
Figures
References
-
- Gulati A, Jabbour A, Ismail TF, Guha K, Khwaja J, Raza S, Morarji K, Brown TD, Ismail NA, Dweck MR, Di Pietro E, Roughton M, Wage R, Daryani Y, O'Hanlon R, Sheppard MN, Alpendurada F, Lyon AR, Cook SA, Cowie MR, Assomull RG, Pennell DJ, Prasad SK. Association of fibrosis with mortality and sudden cardiac death in patients with nonischemic dilated cardiomyopathy. JAMA. 2013; 309:896-908 - PubMed
-
- Butler J, Fonarow GC, Gheorghiade M. Strategies and opportunities for drug development in heart failure. JAMA. 2013; 309:1593-1594 - PubMed
-
- Gheorghiade M, Abraham WT, Albert NM, Greenberg BH, O'Connor CM, She L, Stough WG, Yancy CW, Young JB, Fonarow GC. Systolic blood pressure at admission, clinical characteristics, and outcomes in patients hospitalized with acute heart failure. JAMA. 2006; 296:2217-2226 - PubMed
-
- Gheorghiade M, Vaduganathan M, Fonarow GC, Bonow RO. Rehospitalization for heart failure: problems and perspectives. J Am Coll Cardiol. 2013; 61:391-403 - PubMed
-
- Pang PS, Komajda M, Gheorghiade M. The current and future management of acute heart failure syndromes. Eur Heart J. 2010; 31:784-793 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
