

Minimal access aortic valve replacement via limited skin incision and complete median sternotomy
- PMID: 24251023
- PMCID: PMC3831837
- DOI: 10.3978/j.issn.2072-1439.2013.09.23
Minimal access aortic valve replacement via limited skin incision and complete median sternotomy
Abstract
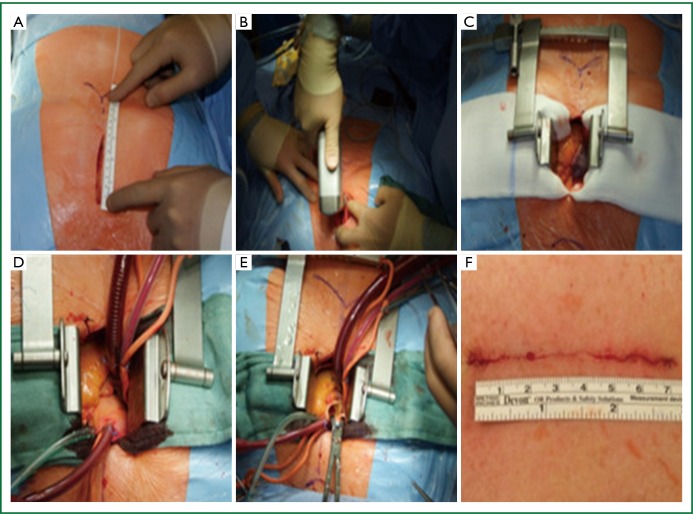
Surgical aortic valve replacement (AVR) via complete median sternotomy is a safe and time-tested technique associated with excellent short- and long-term outcome. Over the last two decades, different minimally-invasive approaches for AVR have been developed and are increasingly being utilized. All these approaches have been developed with the main objective of decreased invasiveness and less surgical trauma. Advantages of minimal invasive AVR have been shown as better cosmesis, shorter ventilation time, decreased blood loss, shorter intensive care unit and hospital length of stay, and less postoperative pain with mortality and morbidity comparable to conventional complete median sternotomy. One well-recognized but less practiced surgical technique for surgical AVR is the complete median sternotomy via limited skin incision. This review article provides a detailed insight into the technical aspects, outcomes, advantages and disadvantages associated with minimal access AVR via limited skin incision and complete median sternotomy.
Keywords: Aortic valve replacement (AVR); limited skin incision; median sternotomy; minimal access surgery; minimally invasive surgery.
Figures
References
-
- Carabello BA, Paulus WJ. Aortic stenosis. Lancet 2009;373:956-66 - PubMed
-
- Schwarz F, Baumann P, Manthey J, et al. Circulation 1982;66:1105-10 - PubMed
-
- Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2008;52:e1-142 - PubMed
-
- Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012): the Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur J Cardiothorac Surg 2012;42:S1-44 - PubMed
-
- Cosgrove DM, 3rd, Sabik JF. Minimally invasive approach for aortic valve operations. Ann Thorac Surg 1996;62:596-7 - PubMed
Publication types
LinkOut - more resources
Full Text Sources