

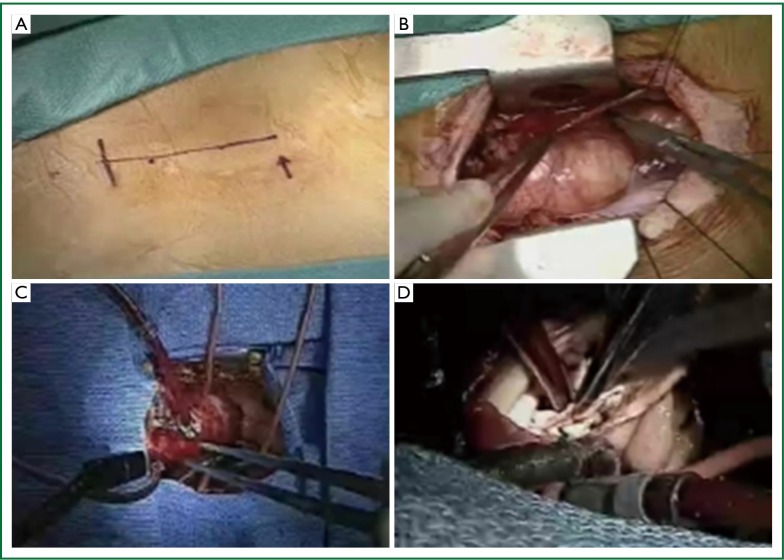
Aortic valve replacement through J-shaped partial upper sternotomy
- PMID: 24251025
- PMCID: PMC3831838
- DOI: 10.3978/j.issn.2072-1439.2013.10.02
Aortic valve replacement through J-shaped partial upper sternotomy
Abstract
The introduction of minimally invasive techniques in general surgery, in the late 1980s, influenced cardiac surgery as well. This led to the emergence of several minimal access approaches for aortic valve replacement (AVR). Currently, the upper partial sternotomy with unilateral J-shaped extension to the right through the fourth intercostal space is the most popular minimal access approach. This approach offers the comfort factor of sternotomy, improved cosmetic result, preserved respiratory mechanics, and last but not the least cost saving as no new equipment is required. On the other hand, inability to visualize the whole heart, adequately de-air the left heart, and failure to apply epicardial pacing wires are some of the perceived disadvantages of this approach. This article provides a comprehensive review of the indications, contraindications, technical aspects, outcomes, advantages and disadvantages of AVR through J-shaped partial upper sternotomy.
Keywords: Aortic valve replacement (AVR); J-shaped limited sternotomy; minimal access surgery; minimally invasive surgery; partial upper sternotomy.
Figures
Similar articles
-
Benefits of rapid deployment aortic valve replacement with a mini upper sternotomy.J Cardiothorac Surg. 2020 Aug 26;15(1):226. doi: 10.1186/s13019-020-01268-y. J Cardiothorac Surg. 2020. PMID: 32847577 Free PMC article.
-
Minimal-access median sternotomy for aortic valve replacement.J Thorac Dis. 2013 Nov;5 Suppl 6(Suppl 6):S650-3. doi: 10.3978/j.issn.2072-1439.2013.10.08. J Thorac Dis. 2013. PMID: 24251022 Free PMC article. Review.
-
[Aortic valve operations through an upper partial sternotomy].Kyobu Geka. 1999 Jul;52(7):519-24; discussion 525-7. Kyobu Geka. 1999. PMID: 10402777 Japanese.
-
Minimal access aortic valve replacement via limited skin incision and complete median sternotomy.J Thorac Dis. 2013 Nov;5 Suppl 6(Suppl 6):S654-7. doi: 10.3978/j.issn.2072-1439.2013.09.23. J Thorac Dis. 2013. PMID: 24251023 Free PMC article. Review.
-
Mini-Bentall: An Interesting Approach for Selected Patients.Innovations (Phila). 2017 Jan/Feb;12(1):41-45. doi: 10.1097/IMI.0000000000000337. Innovations (Phila). 2017. PMID: 28129319
Cited by
-
Partial upper sternotomy for aortic valve replacement provides similar mid-term outcomes as the full sternotomy.J Thorac Dis. 2022 Apr;14(4):857-865. doi: 10.21037/jtd-21-1494. J Thorac Dis. 2022. PMID: 35572904 Free PMC article.
-
Does minimal invasive cardiac surgery reduce the incidence of post-operative atrial fibrillation?Ann Card Anaesth. 2020 Jan-Mar;23(1):7-13. doi: 10.4103/aca.ACA_158_18. Ann Card Anaesth. 2020. PMID: 31929240 Free PMC article. Review.
-
Minimally invasive aortic valve replacement: 12-year single center experience.Ann Cardiothorac Surg. 2015 Mar;4(2):160-9. doi: 10.3978/j.issn.2225-319X.2014.12.05. Ann Cardiothorac Surg. 2015. PMID: 25870812 Free PMC article.
-
Correlation of Preoperative Renal Insufficiency With Mortality and Morbidity After Aortic Valve Replacement: A Propensity Score Matching Analysis.Medicine (Baltimore). 2016 Mar;95(9):e2576. doi: 10.1097/MD.0000000000002576. Medicine (Baltimore). 2016. PMID: 26945348 Free PMC article.
-
Right anterior mini-thoracotomy and sutureless valves: the perfect marriage.Ann Cardiothorac Surg. 2020 Jul;9(4):305-313. doi: 10.21037/acs-2019-surd-172. Ann Cardiothorac Surg. 2020. PMID: 32832412 Free PMC article.
References
-
- Cosgrove DM, 3rd, Sabik JF. Minimally invasive approach for aortic valve operations. Ann Thorac Surg 1996;62:596-7 - PubMed
-
- Benetti FJ, Mariani MA, Rizzardi JL, et al. Minimally invasive aortic valve replacement. J Thorac Cardiovasc Surg 1997;113:806-7 - PubMed
-
- Gundry SR, Shattuck OH, Razzouk AJ, et al. Facile minimally invasive cardiac surgery via ministernotomy. Ann Thorac Surg 1998;65:1100-4 - PubMed
-
- Kim BS, Soltesz EG, Cohn LH. Minimally invasive approaches to aortic valve surgery: Brigham experience. Semin Thorac Cardiovasc Surg 2006;18:148-53 - PubMed
Publication types
LinkOut - more resources
Full Text Sources