

Review
doi: 10.3978/j.issn.2072-1439.2013.09.21.
Reoperative minimal access aortic valve replacement
Affiliations
- PMID: 24251026
- PMCID: PMC3831831
- DOI: 10.3978/j.issn.2072-1439.2013.09.21
Item in Clipboard
Review
Reoperative minimal access aortic valve replacement
J Thorac Dis.
2013 Nov.
Abstract
Reoperative minimal access aortic valve replacement (AVR) is performed through an upper hemisternotomy with peripheral cannulation. This approach limits dissection of mediastinum and especially the left internal mammary artery (LIMA) graft in patients with previous coronary artery bypass grafting (CABG) thus minimizing trauma to the patient. This approach is safe and feasible and may have some benefit over conventional full sternotomy in terms of mortality and morbidity.
Keywords: Minimally invasive surgery; aortic valve replacement (AVR); reoperation.
Figures
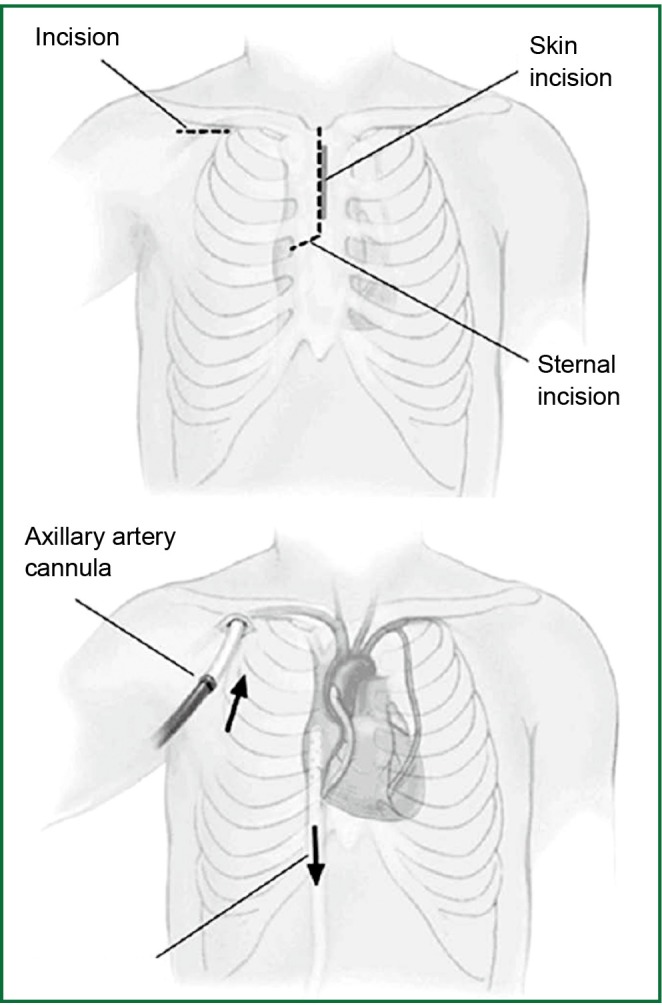
Skin and sternal incision (above) and establishment of cardiopulmonary bypass using right axillary cannulation and percutaneous femoral vein cannulation (below) for reoperative minimally access Aortic Valve Replacement. Reprinted from “Reoperative minimal access aortic valve surgery: minimal mediastinal dissection and minimal injury risk.” Tabata and associates (8). J Thorac Cardiovasc Surg. 2008 with permission from Elsevier.
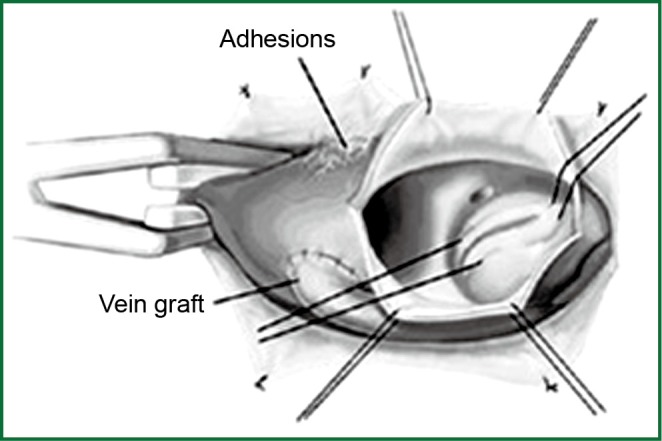
Aortic valve exposure from surgeon’s view. Adhesions are not completely dissected other than cross-clamp site and proximal vein graft anastomosis. Reprinted from “Reoperative minimal access aortic valve surgery: minimal mediastinal dissection and minimal injury risk.” Tabata and associates (8). J Thorac Cardiovasc Surg. 2008 with permission from Elsevier.
References
-
- Brown JM, O’Brien SM, Wu C, et al. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: changes in risks, valve types, and outcomes in the Society of Thoracic Surgeons National Database. J Thorac Cardiovasc Surg 2009;137:82-90 - PubMed
-
- Cosgrove DM, 3rd, Sabik JF. Minimally invasive approach for aortic valve operations. Ann Thorac Surg 1996;62:596-7 - PubMed
-
- Liu J, Sidiropoulos A, Konertz W.Minimally invasive aortic valve replacement (AVR) compared to standard AVR. Eur J Cardiothorac Surg 1999;16Suppl 2:S80-3 - PubMed
-
- Mächler HE, Bergmann P, Anelli-Monti M, et al. Minimally invasive versus conventional aortic valve operations: a prospective study in 120 patients. Ann Thorac Surg 1999;67:1001-5 - PubMed
Publication types
LinkOut - more resources
Full Text Sources