

Minimally invasive approach for redo mitral valve surgery
- PMID: 24251029
- PMCID: PMC3831839
- DOI: 10.3978/j.issn.2072-1439.2013.10.12
Minimally invasive approach for redo mitral valve surgery
Abstract
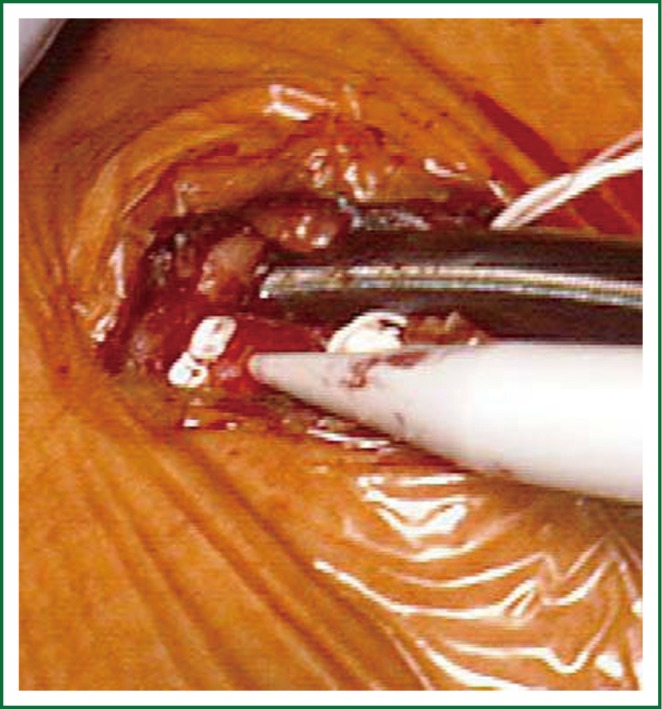
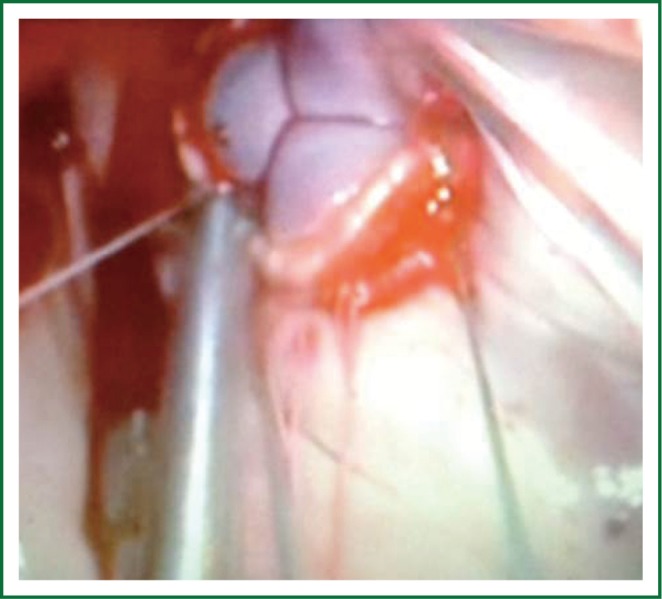
Redo cardiac surgery represents a clinical challenge due to a higher rate of peri-operative morbidity and mortality. Mitral valve re-operations can be particularly demanding in patients with patent coronary artery bypass grafts, previous aortic valve replacement, calcified aorta or complications following a previous operation (abscesses, perivalvular leaks, or thrombosis). Risk of graft injuries, hemorrhage, the presence of dense adhesions and complex valve exposure can make redo valve operations challenging through a median sternotomy. In this review article we provide an overview of minimally invasive approaches for redo mitral valve surgery discussing indications, techniques, outcomes, concerns and controversies. Scientific literature about minimally invasive approach for redo mitral surgery was reviewed with a MEDLINE search strategy combining "mitral valve" with the following terms: 'minimally invasive', 'reoperation', and 'alternative approach'. The search was limited to the last ten years. A total of 168 papers were found using the reported search. From these, ten papers were identified to provide the best evidence on the subject. Mitral valve reoperations can be safely and effectively performed through a smaller right thoracotomy in the fourth intercostal space termed "mini" thoracotomy or "port access". The greatest potential benefit of a right mini-thoracotomy is the avoidance of sternal re-entry and limited dissection of adhesions, avoiding the risk of injury to cardiac structures or patent grafts. Good percentages of valve repair can be achieved. Mortality is low as well as major complications. Minimally invasive procedures with an unclamped aorta have the potential to combine the benefits of minimally invasive access and continuous myocardial perfusion. Less invasive trans-catheter techniques could be considered as the natural future evolution for management of structural heart disease and mitral reoperations. The safety and efficacy of these procedures has never been compared to open reoperations in a randomized trial, although published case series and comparisons to historical cohorts suggest that they are an effective and feasible alternative. Ongoing follow-up on current series will further define these procedures and provide valuable clinical outcome data.
Keywords: Mitral valve; minimally invasive approach; reoperation.
Figures



References
-
- Botta L, Cannata A, Fratto P, et al. The role of the minimally invasive beating heart technique in reoperative valve surgery. J Card Surg 2012;27:24-8 - PubMed
-
- Seeburger J, Borger MA, Falk V, et al. Minimally invasive mitral valve surgery after previous sternotomy: experience in 181 patients. Ann Thorac Surg 2009;87:709-14 - PubMed
-
- Thompson MJ, Behranwala A, Campanella C, et al. Immediate and long-term results of mitral prosthetic replacement using a right thoracotomy beating heart technique. Eur J Cardiothorac Surg 2003;24:47-51; discussion 51 - PubMed
-
- Salhiyyah K, Taggart D.Beating-heart valve surgery: A systematic review. Asian Cardiovasc Thorac Ann 2009;17:650-8 - PubMed
Publication types
LinkOut - more resources
Full Text Sources