

BRAF inhibition is associated with increased clonality in tumor-infiltrating lymphocytes
- PMID: 24251082
- PMCID: PMC3827093
- DOI: 10.4161/onci.26615
BRAF inhibition is associated with increased clonality in tumor-infiltrating lymphocytes
Abstract
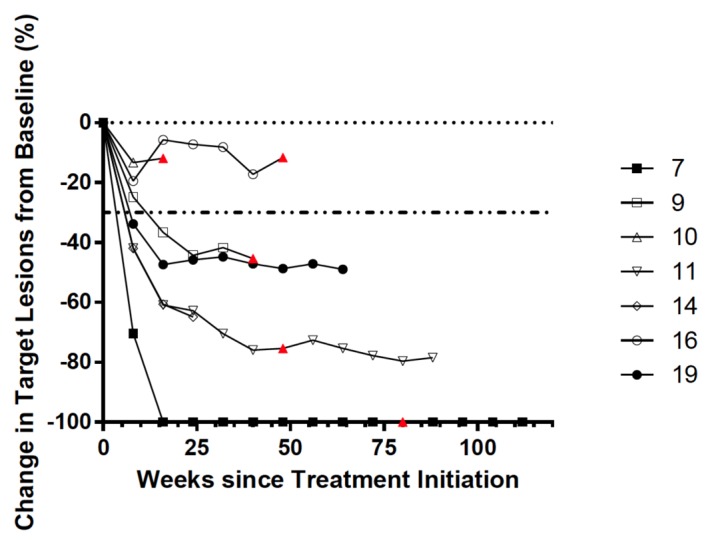
There have been significant advances with regard to BRAF-targeted therapies against metastatic melanoma. However, the majority of patients receiving BRAF inhibitors (BRAFi) manifest disease progression within a year. We have recently shown that melanoma patients treated with BRAFi exhibit an increase in melanoma-associated antigens and in CD8+ tumor-infiltrating lymphocytes in response to therapy. To characterize such a T-cell infiltrate, we analyzed the complementarity-determining region 3 (CDR3) of rearranged T-cell receptor (TCR) β chain-coding genes in tumor biopsies obtained before the initiation of BRAFi and 10-14 d later. We observed an increase in the clonality of tumor-infiltrating lymphocytes in 7 of 8 patients receiving BRAFi, with a statistically significant 21% aggregate increase in clonality. Over 80% of individual T-cell clones detected after initiation of BRAFi treatment were new clones. Interestingly, the comparison of tumor infiltrates with clinical responses revealed that patients who had a high proportion of pre-existing dominant clones after the administration of BRAFi responded better to therapy than patients who had a low proportion of such pre-existing dominant clones following BRAFi. These data suggest that although the inhibition of BRAF in melanoma patients results in tumor infiltration by new lymphocytes, the response to treatment appears to be related to the presence of a pre-existing population of tumor-infiltrating T-cell clones.
Keywords: BRAF; T cells; TILs; melanoma; vemurafenib.
Figures


References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials