

Carotid and vagal body paragangliomas
- PMID: 24251239
- PMCID: PMC3829792
Carotid and vagal body paragangliomas
Abstract
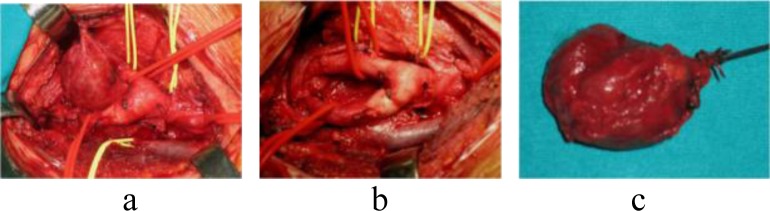
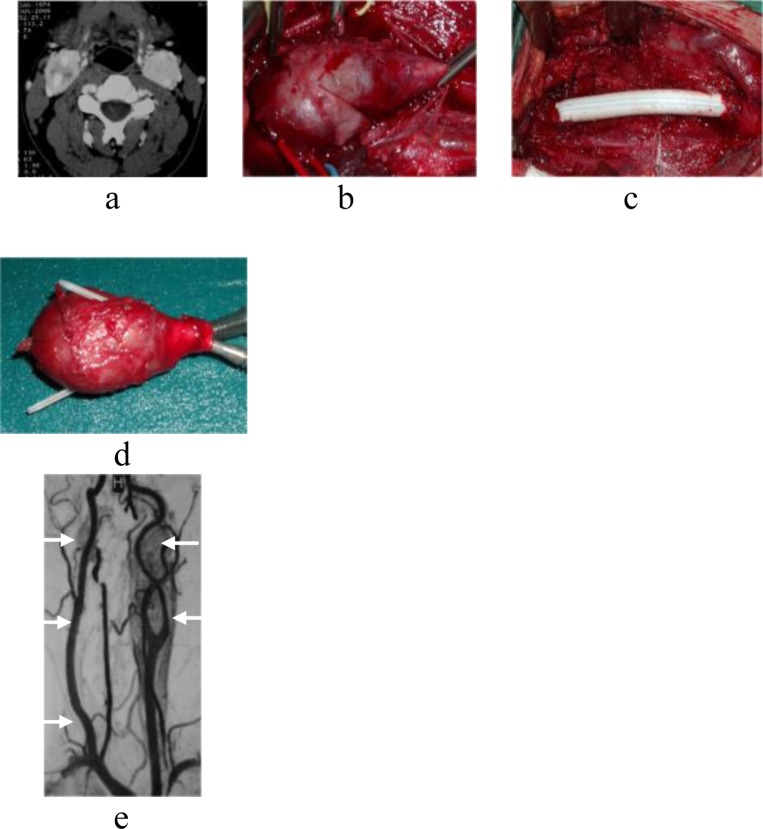
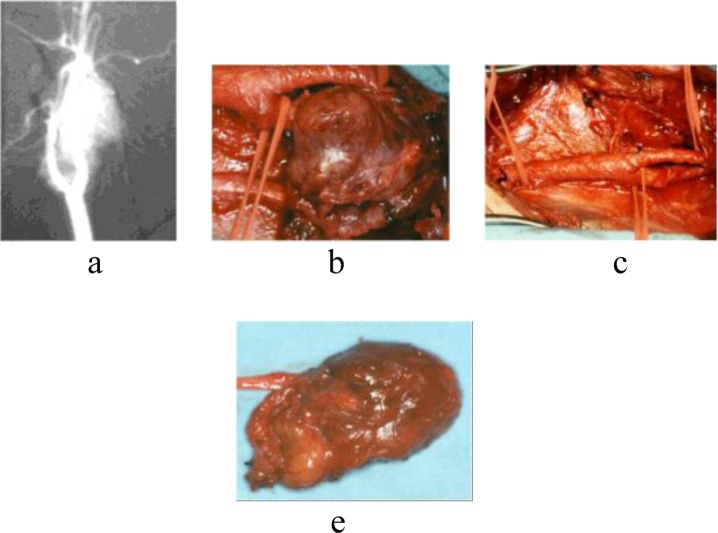
Between 1972 and 2012, 25 patients presenting 32 paragangliomas of the neck were observed. Tumor locations included the carotid body (CBTs) in 21 patients and the vagus nerve in 4. Four patients had bilateral CBT and one a bilateral vagal tumor; a metachronous bilateral jugulare paraganglioma was diagnosed in one patient with bilateral CBT Shamblin type III. Five patients presented CBTs type II and three type III. Preoperative embolization was performed in 5 CBTs, with no significant difference in blood loss. Twenty-nine paragangliomas were resected (with three internal carotid artery resection): there were no cerebrovascular accident or perioperative death. Nine patients (36%) had cranial nerve palsy prior to surgery and a postoperative nerve dysfunction occurred in four other tumors (16%). Persistent nerve deficits occurred in 3 patients (12%). No evidence of malignancy was shown, intraoperatively or during a postoperative follow-up period (9 months to 18 years; mean: 8 years).
Keywords: Carotid body tumor; Vagal paraganglioma.
Figures
References
-
- Garcia MAS , Pendàs JLL , Tapia JPR , Rostàn GG , Fente VS , Pelaz A , Nieto CS . Head and Neck Paragangliomas: Revision of 89 cases in 73 patients . Acta Otorinolaringol Esp . 2007 ; 58 : 94 – 100 . - PubMed
-
- Rodriguez-Cuevas S , Lopez-Garza J , Labastida- Almendaro S . Carotid body tumors in inhabitants of altitudes higher than 2000 meters above sea level . Head Neck . 1998 ; 20 : 374 – 8 . - PubMed
-
- Wang ZY , Bisgard GE . Chronic hyp oxiainducedmorphological and neurochemical changes in the carotid body . Microsc Res Tech . 2002 ; 59 : 168 – 77 . - PubMed
-
- Mhatre AN , Li Y , Gasperin A , Lalwani AK . SDHB, SDHC, and SDHD mutation screen in sporadic and familial head and neck paragangliomas . Clin Genet . 2004 ; 66 : 461 – 6 . - PubMed
-
- Casagranda G , Demattè S , Donner D , Sammartano S , Rozzanigo U , Peterlongo P , Centonze M . Paragangliomas in an endemic area: from genetics to morphofunctional imaging. A pictorial essay . Radiol Med . 2012 ; 117 : 471 – 487 . - PubMed
LinkOut - more resources
Full Text Sources