

A pharmacogenetic versus a clinical algorithm for warfarin dosing
- PMID: 24251361
- PMCID: PMC3942158
- DOI: 10.1056/NEJMoa1310669
A pharmacogenetic versus a clinical algorithm for warfarin dosing
Abstract
Background: The clinical utility of genotype-guided (pharmacogenetically based) dosing of warfarin has been tested only in small clinical trials or observational studies, with equivocal results.
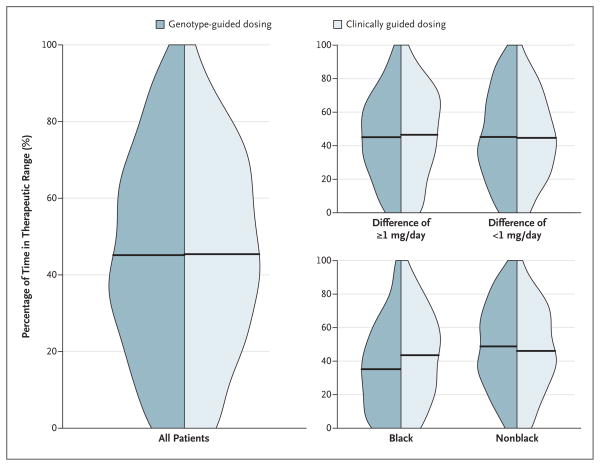
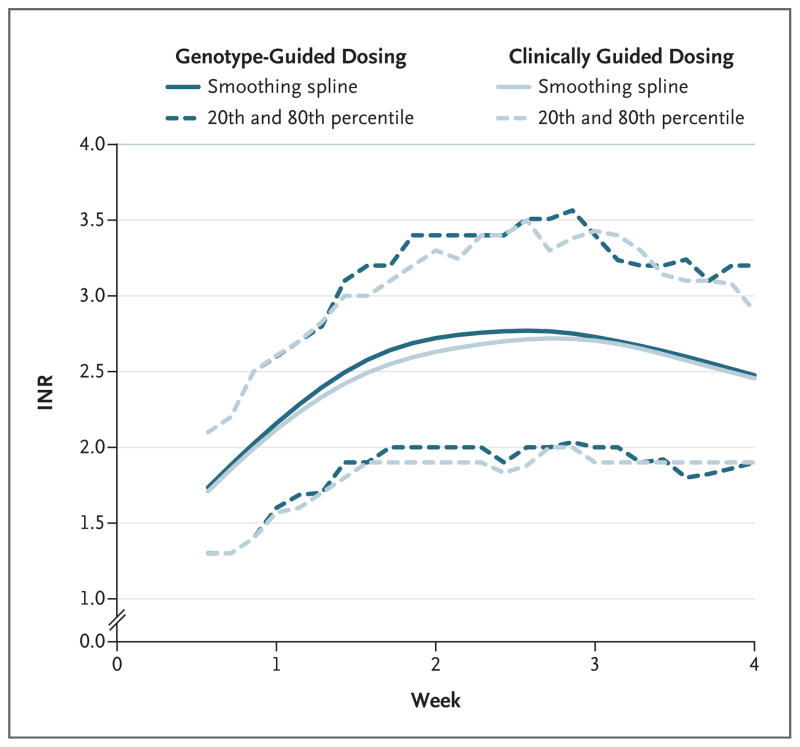
Methods: We randomly assigned 1015 patients to receive doses of warfarin during the first 5 days of therapy that were determined according to a dosing algorithm that included both clinical variables and genotype data or to one that included clinical variables only. All patients and clinicians were unaware of the dose of warfarin during the first 4 weeks of therapy. The primary outcome was the percentage of time that the international normalized ratio (INR) was in the therapeutic range from day 4 or 5 through day 28 of therapy.
Results: At 4 weeks, the mean percentage of time in the therapeutic range was 45.2% in the genotype-guided group and 45.4% in the clinically guided group (adjusted mean difference, [genotype-guided group minus clinically guided group], -0.2; 95% confidence interval, -3.4 to 3.1; P=0.91). There also was no significant between-group difference among patients with a predicted dose difference between the two algorithms of 1 mg per day or more. There was, however, a significant interaction between dosing strategy and race (P=0.003). Among black patients, the mean percentage of time in the therapeutic range was less in the genotype-guided group than in the clinically guided group. The rates of the combined outcome of any INR of 4 or more, major bleeding, or thromboembolism did not differ significantly according to dosing strategy.
Conclusions: Genotype-guided dosing of warfarin did not improve anticoagulation control during the first 4 weeks of therapy. (Funded by the National Heart, Lung, and Blood Institute and others; COAG ClinicalTrials.gov number, NCT00839657.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Do pharmacogenetics have a role in the dosing of vitamin K antagonists?N Engl J Med. 2013 Dec 12;369(24):2345-6. doi: 10.1056/NEJMe1313682. Epub 2013 Nov 19. N Engl J Med. 2013. PMID: 24251364 No abstract available.
-
Anticoagulation therapy: genotype-guided anticoagulation therapy-the jury is still out.Nat Rev Cardiol. 2014 Jan;11(1):1. doi: 10.1038/nrcardio.2013.187. Epub 2013 Dec 3. Nat Rev Cardiol. 2014. PMID: 24302217 No abstract available.
-
Pharmacogenetics and coumarin dosing--recalibrating expectations.N Engl J Med. 2013 Dec 12;369(24):2273-5. doi: 10.1056/NEJMp1314529. N Engl J Med. 2013. PMID: 24328463 No abstract available.
-
Warfarin dosing by genotype did not improve time in therapeutic range.Ann Intern Med. 2014 Mar 18;160(6):JC8. doi: 10.7326/0003-4819-160-6-201403180-02008. Ann Intern Med. 2014. PMID: 24638186 No abstract available.
-
Genotype-guided dosing of vitamin K antagonists.N Engl J Med. 2014 May 1;370(18):1763-4. doi: 10.1056/NEJMc1402521. N Engl J Med. 2014. PMID: 24785213 No abstract available.
-
Genotype-guided dosing of vitamin K antagonists.N Engl J Med. 2014 May 1;370(18):1761. doi: 10.1056/NEJMc1402521. N Engl J Med. 2014. PMID: 24785214 No abstract available.
-
Genotype-guided dosing of vitamin K antagonists.N Engl J Med. 2014 May 1;370(18):1761-2. doi: 10.1056/NEJMc1402521. N Engl J Med. 2014. PMID: 24785215 No abstract available.
-
Genotype-guided dosing of vitamin K antagonists.N Engl J Med. 2014 May 1;370(18):1762. doi: 10.1056/NEJMc1402521. N Engl J Med. 2014. PMID: 24785216 No abstract available.
-
Genotype-guided dosing of vitamin K antagonists.N Engl J Med. 2014 May 1;370(18):1762-3. doi: 10.1056/NEJMc1402521. N Engl J Med. 2014. PMID: 24785217 Free PMC article. No abstract available.
-
Genotype-guided dosing of vitamin K antagonists.N Engl J Med. 2014 May 1;370(18):1763. doi: 10.1056/NEJMc1402521. N Engl J Med. 2014. PMID: 24785218 No abstract available.
-
Why admixture matters in genetically-guided therapy: missed targets in the COAG and EU-PACT trials.P R Health Sci J. 2015 Sep;34(3):175-7. P R Health Sci J. 2015. PMID: 26454897 Free PMC article. No abstract available.
References
-
- Ginsburg GS, Voora D. The long and winding road to warfarin pharmacogenetic testing. J Am Coll Cardiol. 2010;55:2813–5. - PubMed
-
- Woodcock J, Lesko LJ. Pharmacogenetics — tailoring treatment for the outliers. N Engl J Med. 2009;360:811–3. - PubMed
-
- Anderson JL, Horne BD, Stevens SM, et al. Randomized trial of genotype-guided versus standard warfarin dosing in patients initiating oral anticoagulation. Circulation. 2007;116:2563–70. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical