

Diagnosis and management of heart failure with preserved ejection fraction: 10 key lessons
- PMID: 24251461
- PMCID: PMC4347209
- DOI: 10.2174/1573403x09666131117131217
Diagnosis and management of heart failure with preserved ejection fraction: 10 key lessons
Abstract
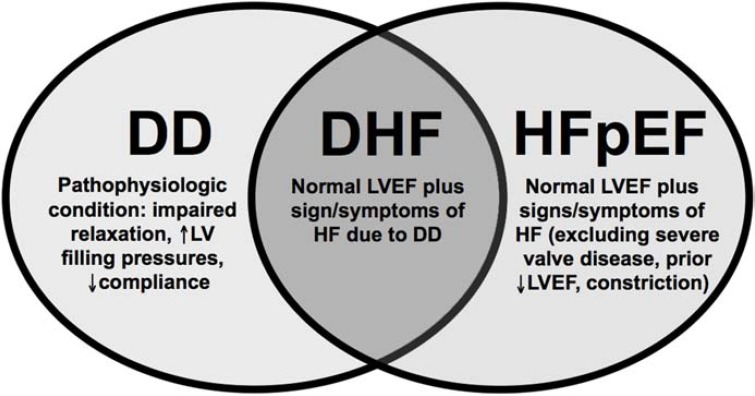
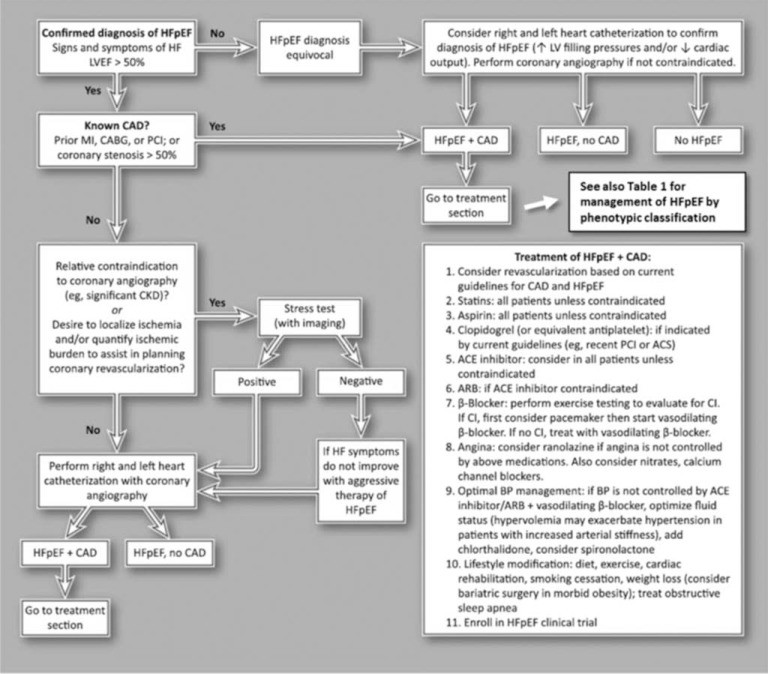
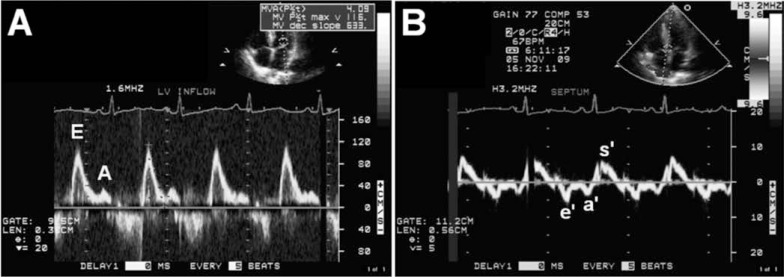
Heart failure with preserved ejection fraction (HFpEF) is a common clinical syndrome associated with high rates of morbidity and mortality. Due to the lack of evidence-based therapies and increasing prevalence of HFpEF, clinicians are often confronted with these patients and yet have little guidance on how to effectively diagnose and manage them. Here we offer 10 key lessons to assist with the care of patients with HFpEF: (1) Know the difference between diastolic dysfunction, diastolic heart failure, and HFpEF; (2) diagnosing HFpEF is challenging, so be thorough and consider invasive hemodynamic testing to confirm the diagnosis; (3) a normal B-type natriuretic peptide does not exclude the diagnosis of HFpEF; (4) elevated pulmonary artery systolic pressure on echocardiography in the presence of a normal ejection fraction should prompt consideration of HFpEF; (5) use dynamic testing in evaluating the possibility of HFpEF in patients with unexplained dyspnea or exercise tolerance; (6) all patients with HFpEF should be systematically evaluated for the presence of coronary artery disease; (7) use targeted treatment for HFpEF patients based on their phenotypic classification; (8) treat HFpEF patients now by treating their comorbidities; (9) understand the importance of heart rate in HFpEF- lower is not always better; and (10) do not forget to consider rare diseases ("zebras") as causes for HFpEF when evaluating and treating patients. Taken together, these 10 key lessons can help clinicians care for challenging patients with HFpEF while we eagerly await the results of ongoing HFpEF clinical trials and observational studies.
Figures
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–9. - PubMed
-
- Steinberg BA, Zhao X, Heidenreich PA , et al. Trends in patients hospitalized with heart failure and preserved left ventricu-lar ejection fraction prevalence, therapies, and outcomes. Circulation. 2012;126:65–75. - PubMed
-
- Bhatia RS, Tu JV, Lee DS , et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med. 2006;355:260–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
