

Live liver donors' risk thresholds: risking a life to save a life
- PMID: 24251593
- PMCID: PMC4048078
- DOI: 10.1111/hpb.12192
Live liver donors' risk thresholds: risking a life to save a life
Abstract
Background: There is still some controversy regarding the ethical issues involved in live donor liver transplantation (LDLT) and there is uncertainty on the range of perioperative morbidity and mortality risks that donors will consider acceptable.
Methods: This study analysed donors' inclinations towards LDLT using decision analysis techniques based on the probability trade-off (PTO) method. Adult individuals with an emotional or biological relationship with a patient affected by end-stage liver disease were enrolled. Of 122 potential candidates, 100 were included in this study.
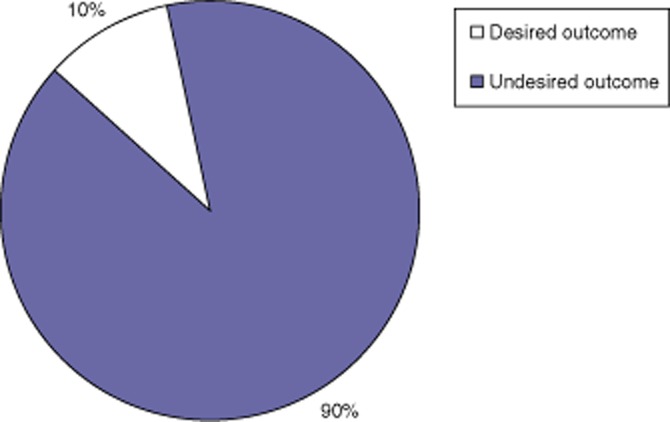
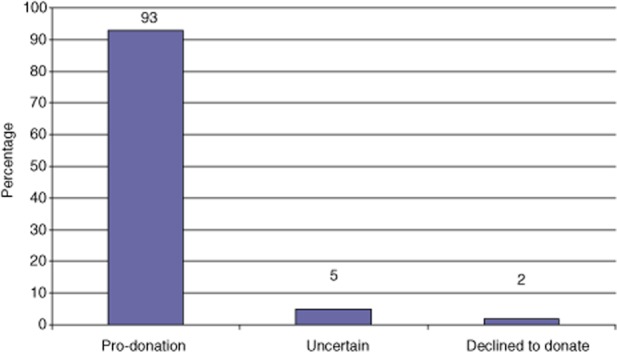
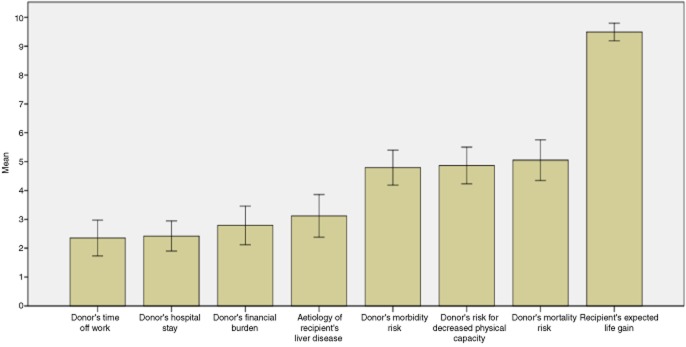
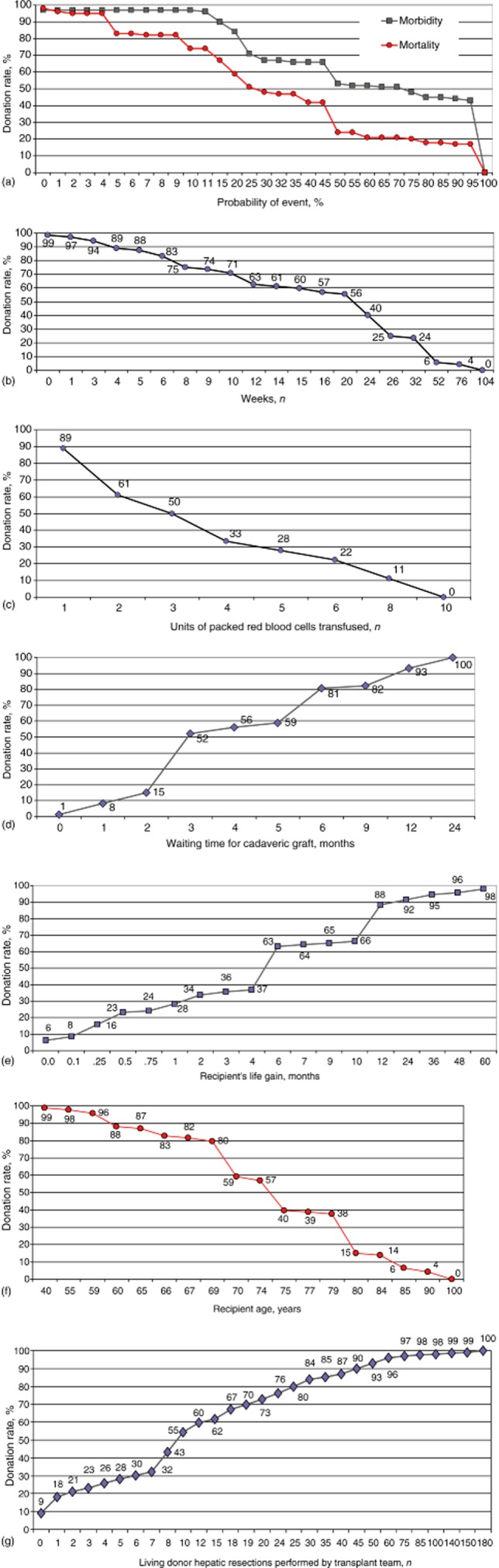
Results: The vast majority of participants (93%) supported LDLT. The most important factor influencing participants' decisions was their wish to improve the recipient's chance of living a longer life. Participants chose to become donors if the recipient was required to wait longer than a mean ± standard deviation (SD) of 6 ± 5 months for a cadaveric graft, if the mean ± SD probability of survival was at least 46 ± 30% at 1 month and at least 36 ± 29% at 1 year, and if the recipient's life could be prolonged for a mean ± SD of at least 11 ± 22 months.
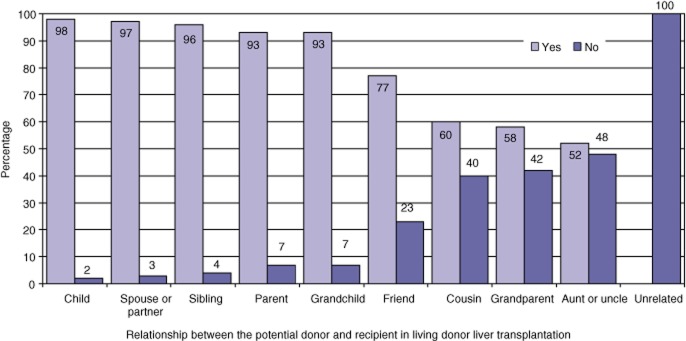
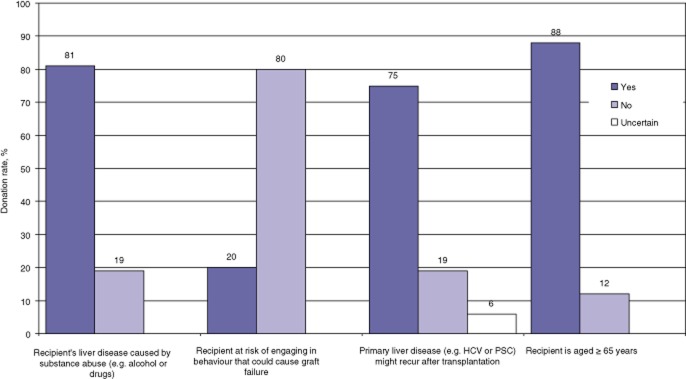
Conclusions: Potential donors were risk takers and were willing to donate when given the opportunity. They accepted significant risks, especially if they had a close emotional relationship with the recipient.
© 2013 International Hepato-Pancreato-Biliary Association.
Figures

References
-
- Kim WR, Brown RS, Jr, Terrault NA, El-Serag H. Burden of liver disease in the United States: summary of a workshop. Hepatology. 2002;36:227–242. - PubMed
-
- Gill JS, Klarenbach S, Cole E, Shemie SD. Deceased organ donation in Canada: an opportunity to heal a fractured system. Am J Transplant. 2008;8:1580–1587. - PubMed
-
- Scientific Registry of Transplant Recipients/Organ Procurement and Transplantation Network. SRTR/OPTN Annual Report. 2009 Available at http://www.ustransplant.org/annual_reports/current/ (last accessed 23 July 2011)
-
- Molinari M, Renfrew PD, Petrie NM, De Coutere S, Abdolell M. Clinical epidemiological analysis of the mortality rate of liver transplant candidates living in rural areas. Transpl Int. 2011;24:292–299. - PubMed
-
- Barshes NR, Horwitz IB, Franzini L, Vierling JM, Goss JA. Waitlist mortality decreases with increased use of extended criteria donor liver grafts at adult liver transplant centres. Am J Transplant. 2007;7:1265–1270. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
