

Improving chronic disease prevention and screening in primary care: results of the BETTER pragmatic cluster randomized controlled trial
- PMID: 24252125
- PMCID: PMC4225577
- DOI: 10.1186/1471-2296-14-175
Improving chronic disease prevention and screening in primary care: results of the BETTER pragmatic cluster randomized controlled trial
Abstract
Background: Primary care provides most of the evidence-based chronic disease prevention and screening services offered by the healthcare system. However, there remains a gap between recommended preventive services and actual practice. This trial (the BETTER Trial) aimed to improve preventive care of heart disease, diabetes, colorectal, breast and cervical cancers, and relevant lifestyle factors through a practice facilitation intervention set in primary care.
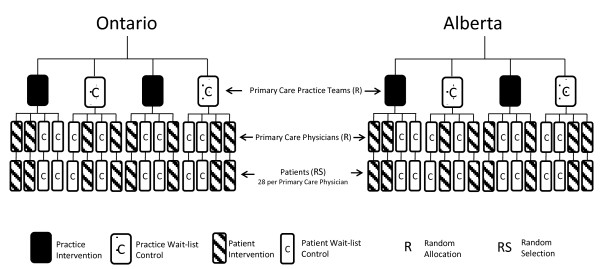
Methods: Pragmatic two-way factorial cluster RCT with Primary Care Physicians' practices as the unit of allocation and individual patients as the unit of analysis. The setting was urban Primary Care Team practices in two Canadian provinces. Eight Primary Care Team practices were randomly assigned to receive the practice-level intervention or wait-list control; 4 physicians in each team (32 physicians) were randomly assigned to receive the patient-level intervention or wait-list control. Patients randomly selected from physicians' rosters were stratified into two groups: 1) general and 2) moderate mental illness. The interventions involved a multifaceted, evidence-based, tailored practice-level intervention with a Practice Facilitator, and a patient-level intervention involving a one-hour visit with a Prevention Practitioner where patients received a tailored 'prevention prescription'. The primary outcome was a composite Summary Quality Index of 28 evidence-based chronic disease prevention and screening actions with pre-defined targets, expressed as the ratio of eligible actions at baseline that were met at follow-up. A cost-effectiveness analysis was conducted.
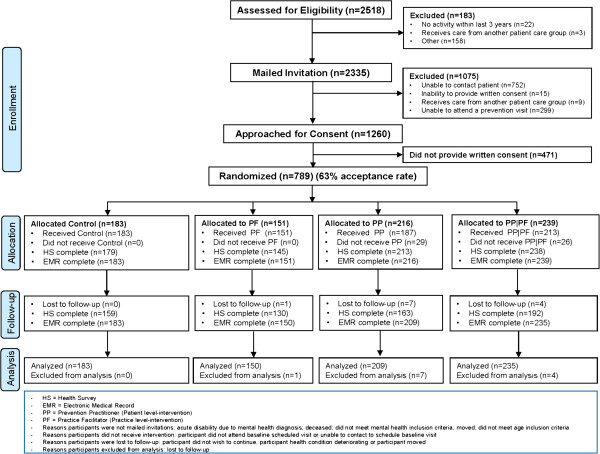
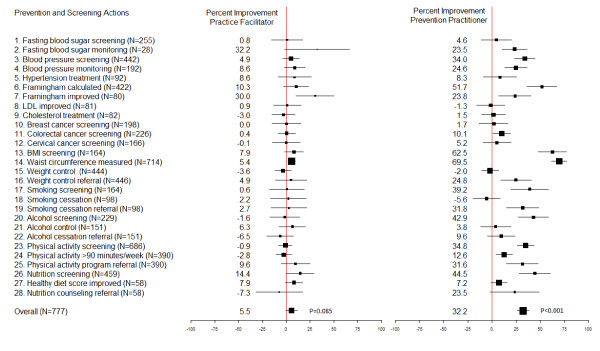
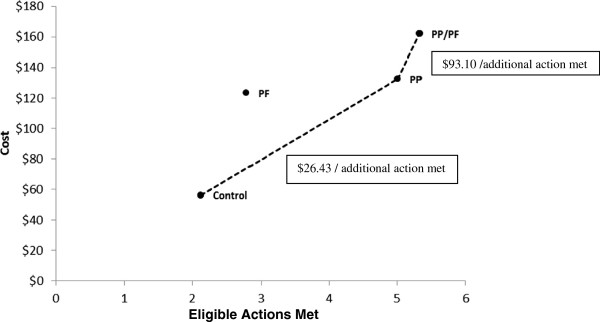
Results: 789 of 1,260 (63%) eligible patients participated. On average, patients were eligible for 8.96 (SD 3.2) actions at baseline. In the adjusted analysis, control patients met 23.1% (95% CI: 19.2% to 27.1%) of target actions, compared to 28.5% (95% CI: 20.9% to 36.0%) receiving the practice-level intervention, 55.6% (95% CI: 49.0% to 62.1%) receiving the patient-level intervention, and 58.9% (95% CI: 54.7% to 63.1%) receiving both practice- and patient-level interventions (patient-level intervention versus control, P < 0.001). The benefit of the patient-level intervention was seen in both strata. The extra cost of the intervention was $26.43CAN (95% CI: $16 to $44) per additional action met.
Conclusions: A Prevention Practitioner can improve the implementation of clinically important prevention and screening for chronic diseases in a cost-effective manner.
Figures
References
-
- Bodenheimer T, Berry-Millett R. Care Management of Patients With Complex Health Care Needs. Princeton (NJ) Robert Wood Johnson Foundation: The Synthesis Project; 2009. - PubMed
-
- Preventing chronic diseases: a vital investment. http://www.who.int/chp/chronic_disease_report/full_report.pdf.
-
- U.S. Preventive services task force home page. http://www.uspreventiveservicestaskforce.org/index.html.
-
- National institute for health and clinical excellence. http://www.nice.org.uk.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
