

Neurological outcomes in patients transported to hospital without a prehospital return of spontaneous circulation after cardiac arrest
- PMID: 24252433
- PMCID: PMC4057418
- DOI: 10.1186/cc13121
Neurological outcomes in patients transported to hospital without a prehospital return of spontaneous circulation after cardiac arrest
Abstract
Introduction: As emergency medical services (EMS) personnel in Japan are not allowed to perform termination of resuscitation in the field, most patients experiencing an out-of-hospital cardiac arrest (OHCA) are transported to hospitals without a prehospital return of spontaneous circulation (ROSC). As the crucial prehospital factors for outcomes are not clear in patients who had an OHCA without a prehospital ROSC, we aimed to determine the prehospital factors associated with 1-month favorable neurological outcomes (Cerebral Performance Category scale 1 or 2 (CPC 1-2)).
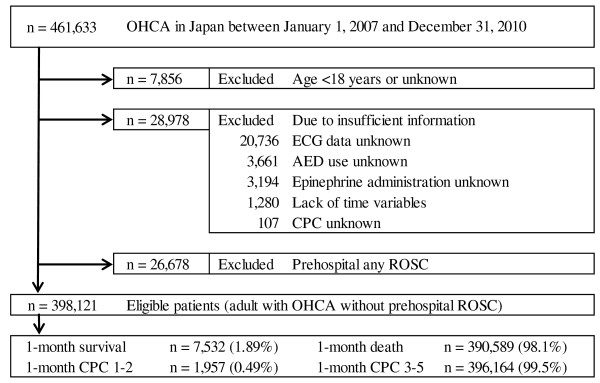
Methods: We analyzed the data of 398,121 adult OHCA patients without a prehospital ROSC from a prospectively recorded nationwide Utstein-style Japanese database from 2007 to 2010. The primary endpoint was 1-month CPC 1-2.
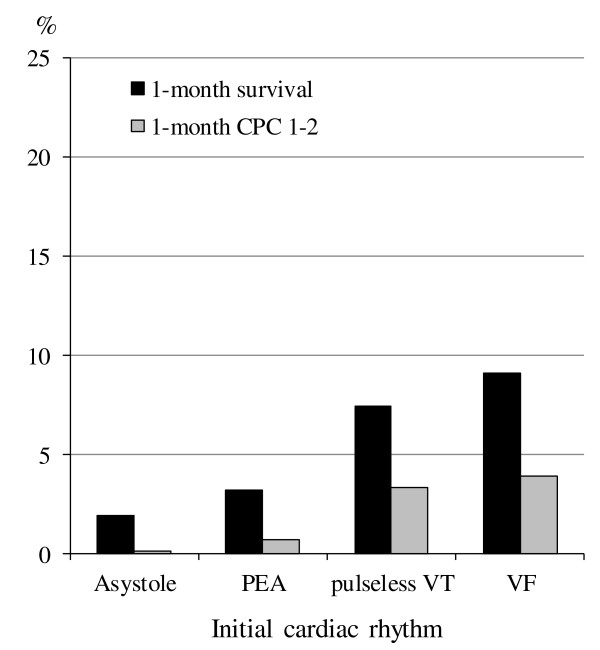
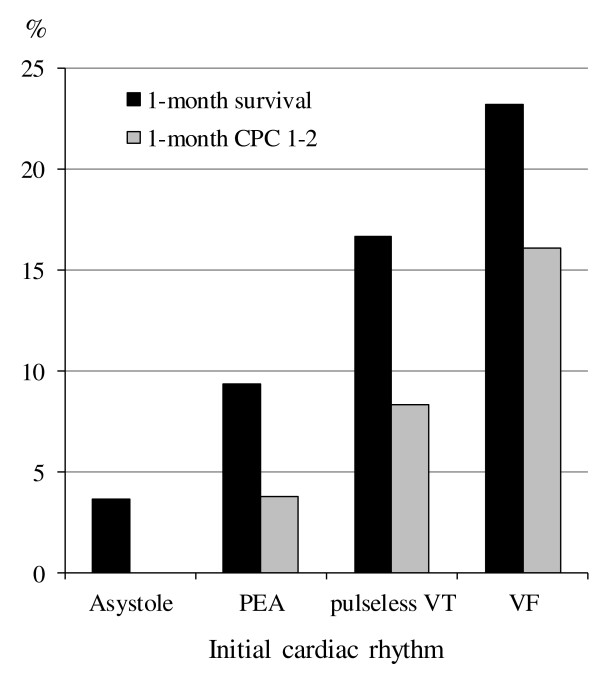
Results: The rate of 1-month CPC 1-2 was 0.49%. Multivariate logistic regression analysis indicated that the independent variables associated with CPC 1-2 were the following nine prehospital factors: (1) initial non-asystole rhythm (ventricular fibrillation (VF): adjusted odds ratio (aOR), 9.37; 95% confidence interval (CI), 7.71 to 11.4; pulseless ventricular tachycardia (VT): aOR, 8.50; 95% CI, 5.36 to 12.9; pulseless electrical activity (PEA): aOR, 2.75; 95% CI, 2.40 to 3.15), (2) age <65 years (aOR, 3.90; 95% CI, 3.28 to 4.67), (3) arrest witnessed by EMS personnel (aOR, 2.82; 95% CI, 2.48 to 3.19), (4) call-to-hospital arrival time <24 minutes (aOR, 2.58; 95% CI, 2.22 to 3.01), (5) arrest witnessed by any layperson, (6) physician-staffed ambulance, (7) call-to-response time <5 minutes, (8) prehospital shock delivery, and (9) presumed cardiac cause. When four crucial key factors (with an aOR >2.0 in the regression model: initial non-asystole rhythm, age <65 years, EMS-witnessed arrest, and call-to-hospital arrival time <24 minutes) were present, the rates of 1-month CPC 1-2 and 1-month survival were 16.1% and 23.2% in initial VF, 8.3% and 16.7% in pulseless VT, and 3.8% and 9.4% in PEA, respectively.
Conclusions: In OHCA patients transported to hospitals without a prehospital ROSC, nine prehospital factors were significantly associated with 1-month CPC 1-2. Of those, four are crucial key factors: initial non-asystole rhythm, age <65 years, EMS-witnessed arrest, and call-to-hospital arrival time <24 minutes.
Figures
References
-
- Kitamura T, Iwami T, Kawamura T, Nagao K, Tanaka H, Hiraide A. Hiraide A for the Implementation Working Group for All-Japan Utstein Registry of the Fire and Disaster Management Agency: Nationwide public access defibrillation in Japan. N Engl J Med. 2010;17:994–1004. doi: 10.1056/NEJMoa0906644. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
