

Comparative utility of LC3, p62 and TDP-43 immunohistochemistry in differentiation of inclusion body myositis from polymyositis and related inflammatory myopathies
- PMID: 24252466
- PMCID: PMC3893502
- DOI: 10.1186/2051-5960-1-29
Comparative utility of LC3, p62 and TDP-43 immunohistochemistry in differentiation of inclusion body myositis from polymyositis and related inflammatory myopathies
Abstract
Background: Inclusion body myositis (IBM) is a slowly progressive inflammatory myopathy of the elderly that does not show significant clinical improvement in response to steroid therapy. Distinguishing IBM from polymyositis (PM) is clinically important since PM is steroid-responsive; however, the two conditions can show substantial histologic overlap.
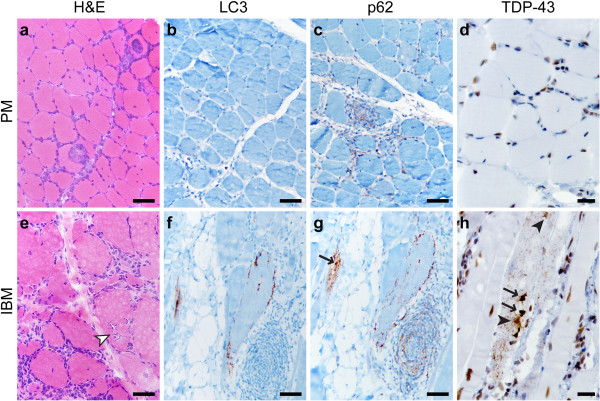
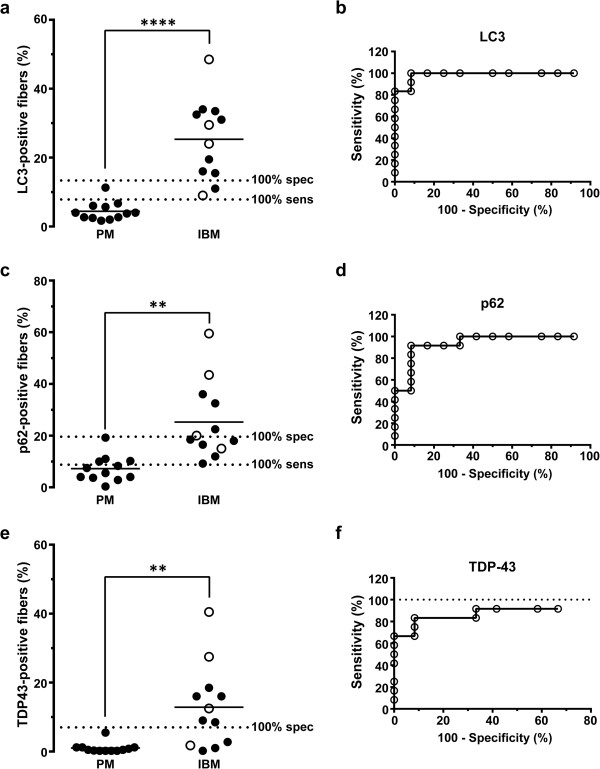
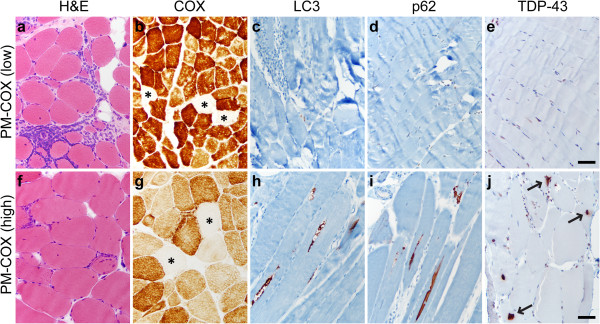
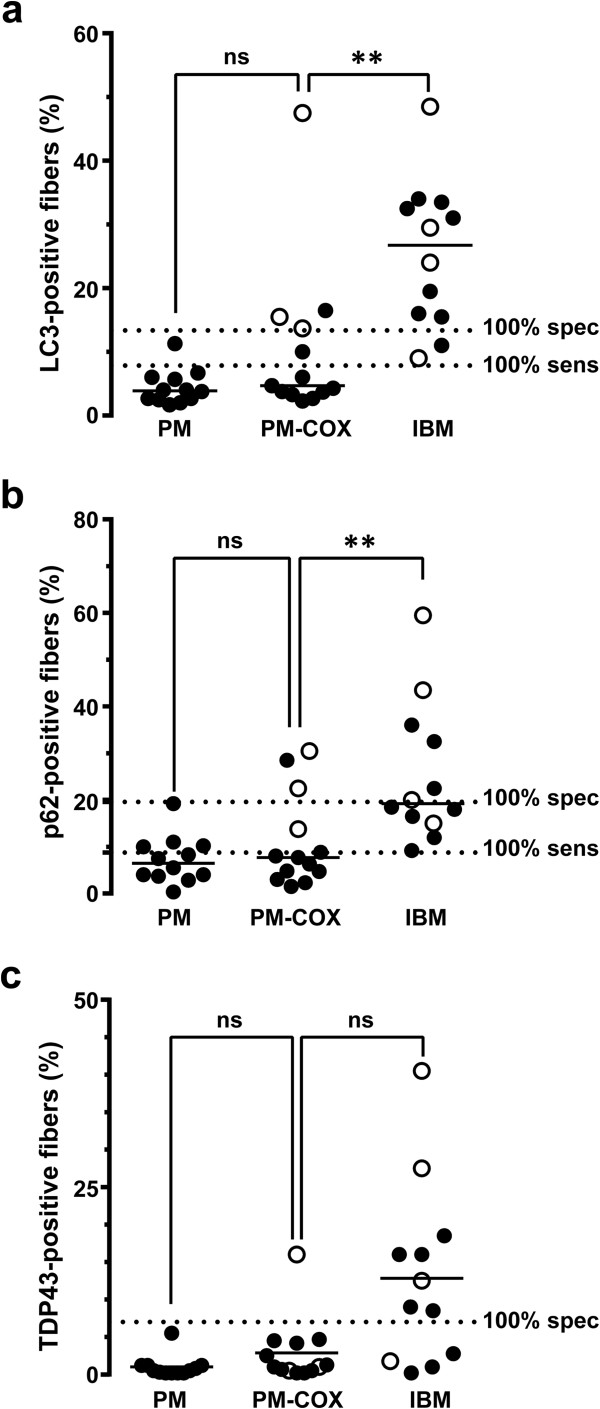
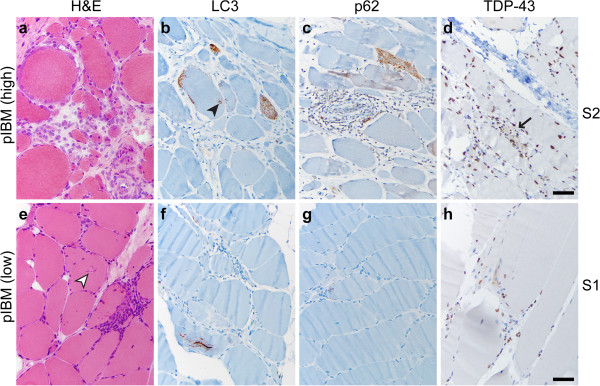
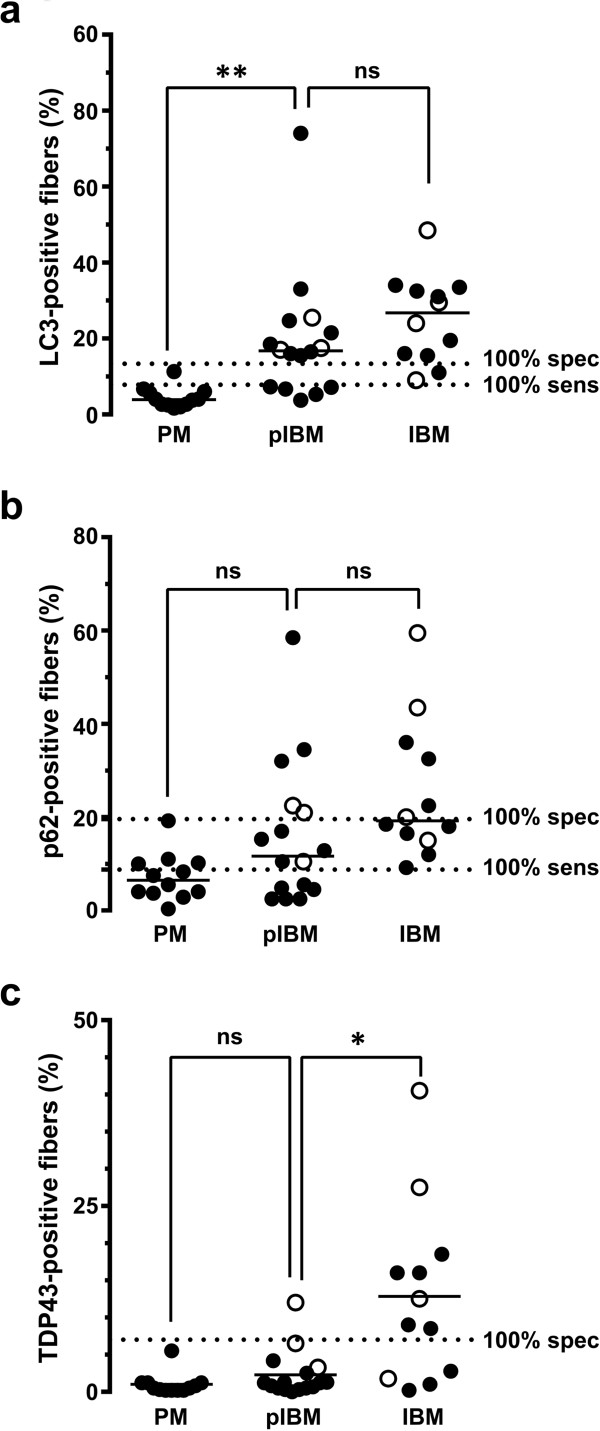
Results: We performed quantitative immunohistochemistry for (1) autophagic markers LC3 and p62 and (2) protein aggregation marker TDP-43 in 53 subjects with pathologically diagnosed PM, IBM, and two intermediate T cell-mediated inflammatory myopathies (polymyositis with COX-negative fibers and possible IBM). The percentage of stained fibers was significantly higher in IBM than PM for all three immunostains, but the markers varied in sensitivity and specificity. In particular, both LC3 and p62 were sensitive markers of IBM, but the tradeoff between sensitivity and specificity was smaller (and diagnostic utility thus greater) for LC3 than for p62. In contrast, TDP-43 immunopositivity was highly specific for IBM, but the sensitivity of this test was low, with definitive staining present in just 67% of IBM cases.
Conclusions: To differentiate IBM from PM, we thus recommend using a panel of LC3 and TDP-43 antibodies: the finding of <14% LC3-positive fibers helps exclude IBM, while >7% of TDP-43-positive fibers strongly supports a diagnosis of IBM. These data provide support for the hypothesis that disruption of autophagy and protein aggregation contribute to IBM pathogenesis.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
