

ECG-based gating in ultra high field cardiovascular magnetic resonance using an independent component analysis approach
- PMID: 24252594
- PMCID: PMC4174900
- DOI: 10.1186/1532-429X-15-104
ECG-based gating in ultra high field cardiovascular magnetic resonance using an independent component analysis approach
Abstract
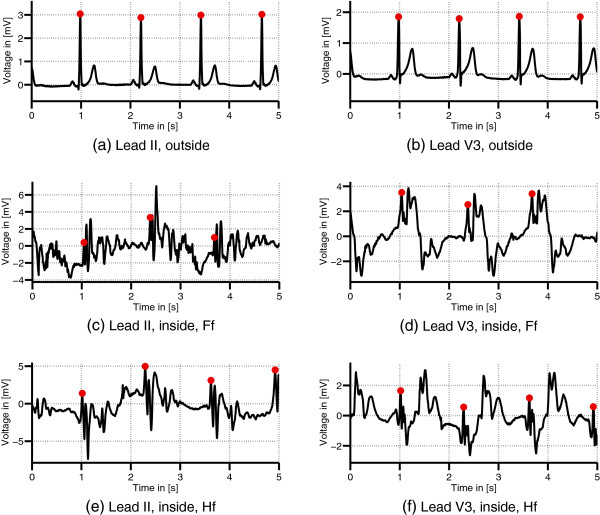
Background: In Cardiovascular Magnetic Resonance (CMR), the synchronization of image acquisition with heart motion is performed in clinical practice by processing the electrocardiogram (ECG). The ECG-based synchronization is well established for MR scanners with magnetic fields up to 3 T. However, this technique is prone to errors in ultra high field environments, e.g. in 7 T MR scanners as used in research applications. The high magnetic fields cause severe magnetohydrodynamic (MHD) effects which disturb the ECG signal. Image synchronization is thus less reliable and yields artefacts in CMR images.
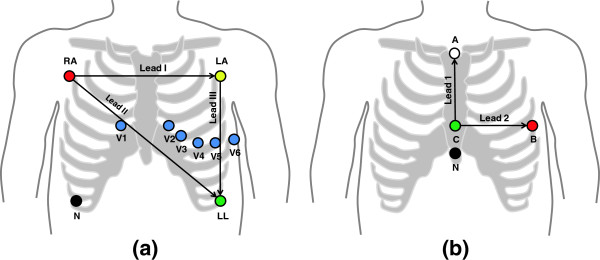
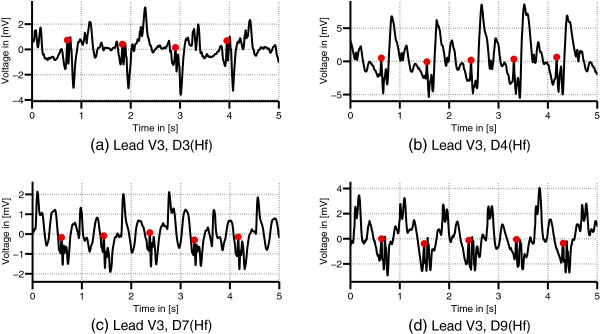
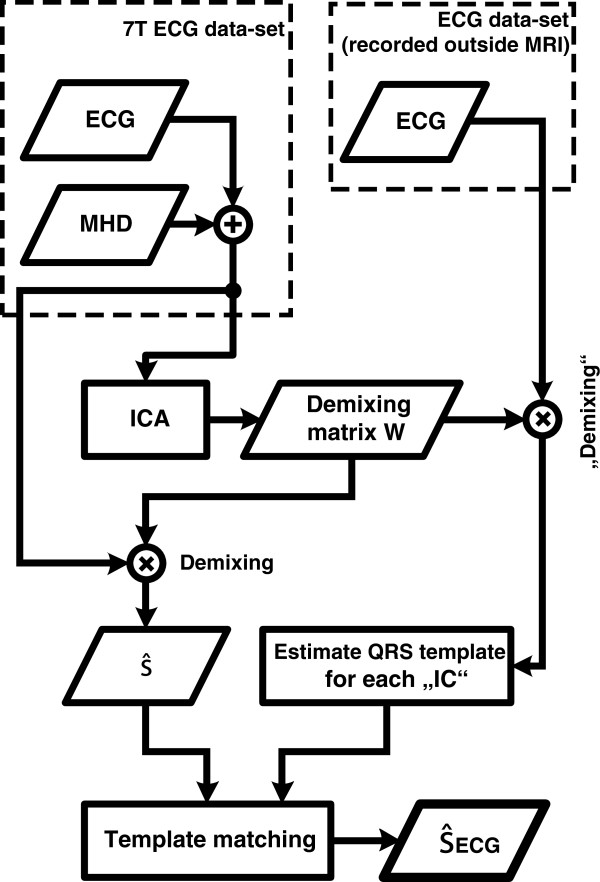
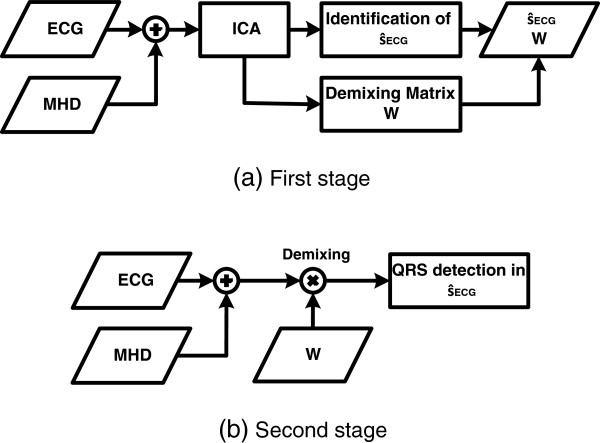
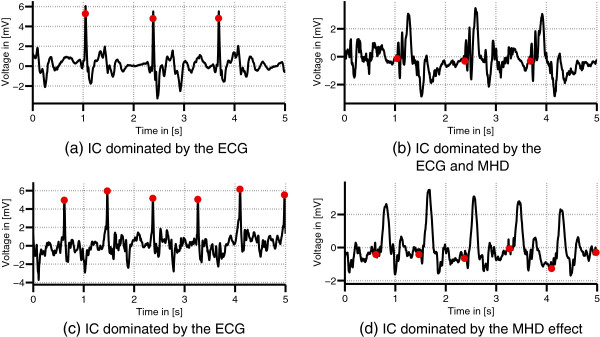
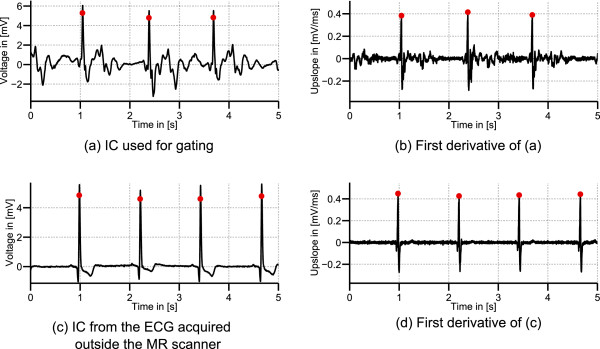
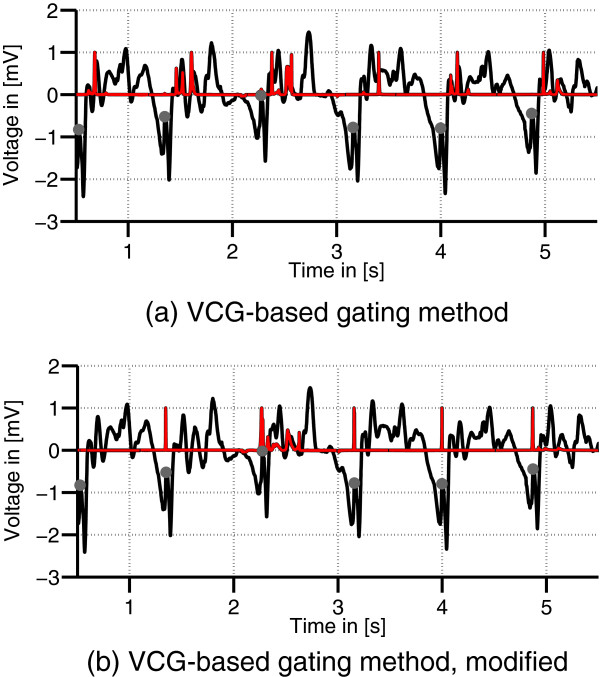
Methods: A strategy based on Independent Component Analysis (ICA) was pursued in this work to enhance the ECG contribution and attenuate the MHD effect. ICA was applied to 12-lead ECG signals recorded inside a 7 T MR scanner. An automatic source identification procedure was proposed to identify an independent component (IC) dominated by the ECG signal. The identified IC was then used for detecting the R-peaks. The presented ICA-based method was compared to other R-peak detection methods using 1) the raw ECG signal, 2) the raw vectorcardiogram (VCG), 3) the state-of-the-art gating technique based on the VCG, 4) an updated version of the VCG-based approach and 5) the ICA of the VCG.
Results: ECG signals from eight volunteers were recorded inside the MR scanner. Recordings with an overall length of 87 min accounting for 5457 QRS complexes were available for the analysis. The records were divided into a training and a test dataset. In terms of R-peak detection within the test dataset, the proposed ICA-based algorithm achieved a detection performance with an average sensitivity (Se) of 99.2%, a positive predictive value (+P) of 99.1%, with an average trigger delay and jitter of 5.8 ms and 5.0 ms, respectively. Long term stability of the demixing matrix was shown based on two measurements of the same subject, each being separated by one year, whereas an averaged detection performance of Se = 99.4% and +P = 99.7% was achieved.Compared to the state-of-the-art VCG-based gating technique at 7 T, the proposed method increased the sensitivity and positive predictive value within the test dataset by 27.1% and 42.7%, respectively.
Conclusions: The presented ICA-based method allows the estimation and identification of an IC dominated by the ECG signal. R-peak detection based on this IC outperforms the state-of-the-art VCG-based technique in a 7 T MR scanner environment.
Figures
References
-
- van Ooij P, Kleinloog R, Zwanenburg J, Visser F, Luijten P, Barker A, Markl M, Nederveen A, Majoie C, Regli L. et al. Improved depiction of hemodynamics in intracranial aneurysms by 4D flow MRI at 7T compared to 3T. J Cardiovasc Magn Reson. 2013;15(Suppl 1):W12. doi: 10.1186/1532-429X-15-S1-W12. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
