

Lipid accumulation, lipid oxidation, and low plasma levels of acquired antibodies against oxidized lipids associate with degeneration and rupture of the intracranial aneurysm wall
- PMID: 24252658
- PMCID: PMC3893371
- DOI: 10.1186/2051-5960-1-71
Lipid accumulation, lipid oxidation, and low plasma levels of acquired antibodies against oxidized lipids associate with degeneration and rupture of the intracranial aneurysm wall
Abstract
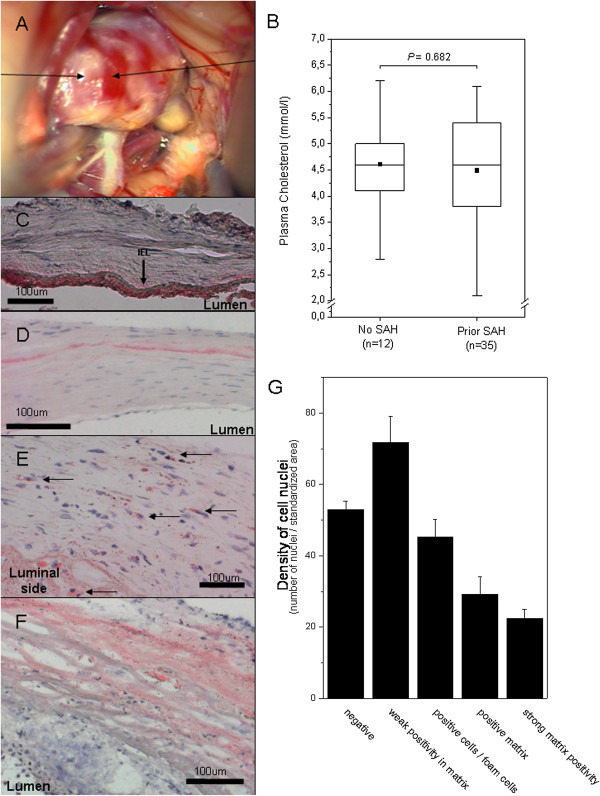
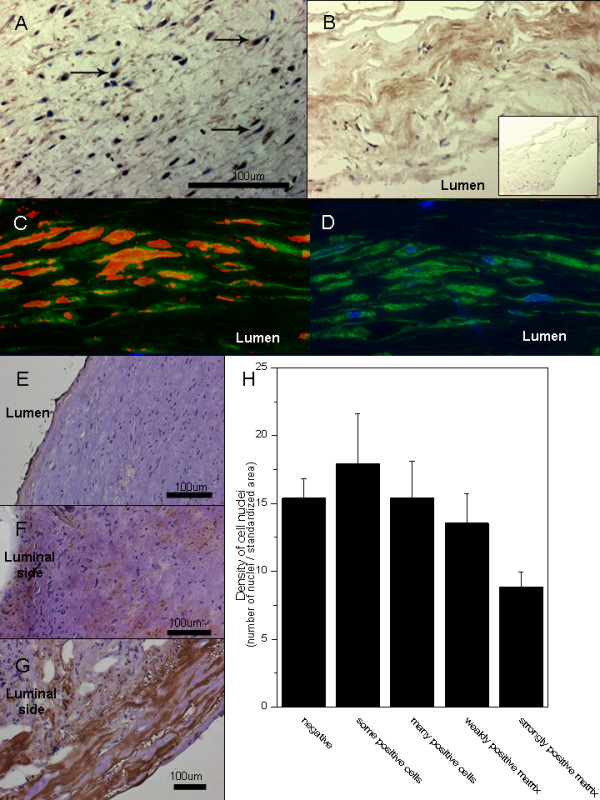
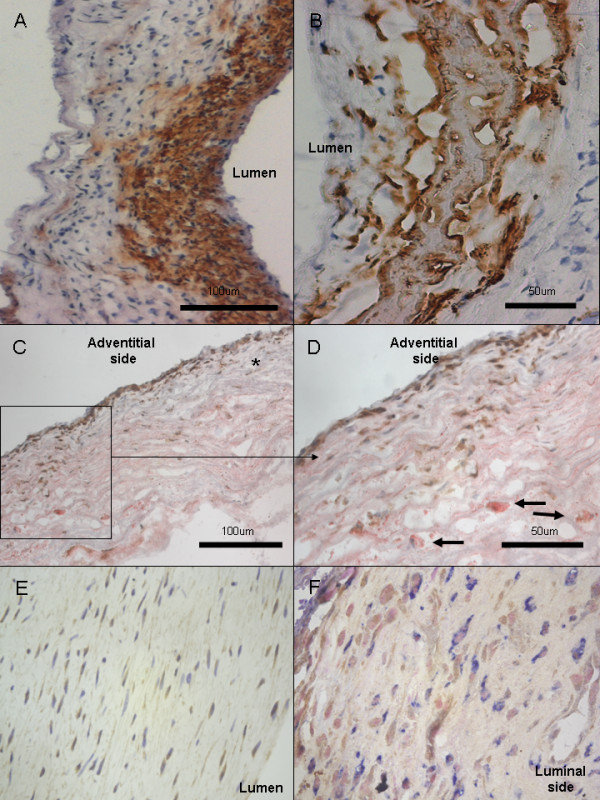
Background: Rupture of a saccular intracranial aneurysm (sIA) causes an often fatal subarachnoid hemorrhage (SAH). Why some sIAs rupture remains unknown. Since sIA walls bear some histological similarities with early atherosclerotic lesions, we hypothesized that accumulation and oxidation of lipids might occur in the sIA wall and might associate with sIA wall degeneration. Tissue samples from sIA fundi (n = 54) were studied with histochemistry and a panel of previously characterized antibodies for epitopes of oxidized LDL (OxLDL). Plasma samples from sIA carriers (n = 125) were studied with ELISA and EIA for IgG and IgM -antibodies against a panel of OxLDL epitopes.
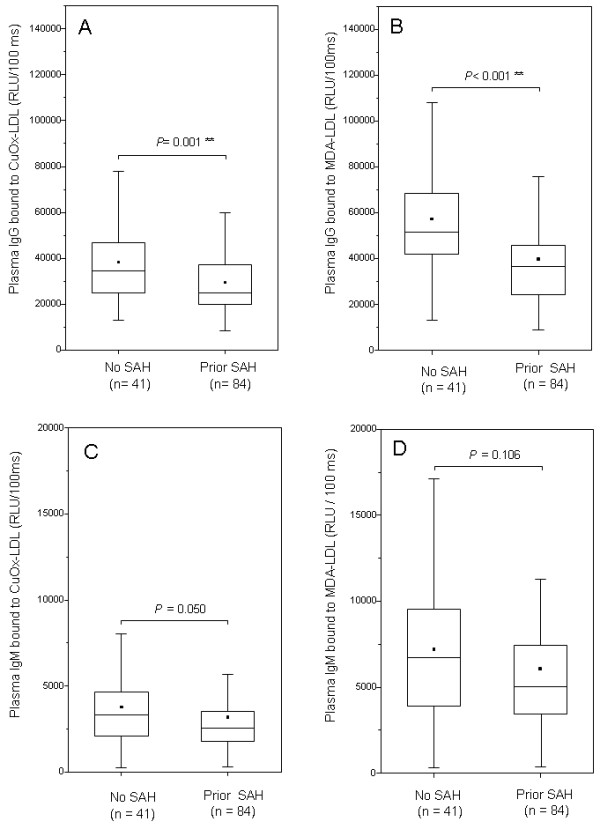
Results: Lipid accumulation, foam cells, and oxidized lipids were found both in unruptured and ruptured sIA walls. Lipid accumulation associated with wall degeneration (P < 0.001), as did the expression of adipophilin, a marker of lipid ingestion by cells. Lipid accumulation associated also with loss of mural cells (P < 0.001), as did the accumulation of OxLDL (P < 0.001). Plasma IgG antibody titers against OxLDL or malondialdehyde modified LDL were higher in patients with unruptured sIAs than in patients with aneurysmal SAH (P ≤ 0.001). A trend but not statistically significant differences were found in plasma IgM antibodies against oxidized lipids.
Conclusions: Accumulation of lipids and their oxidation in the sIA wall associates with the degeneration of the sIA wall. Acquired immunity against oxidized lipid epitopes may be protective of lipid associated sIA wall degeneration, but warrants further studies.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
