

Kaposiform lymphangiomatosis: a distinct aggressive lymphatic anomaly
- PMID: 24252784
- PMCID: PMC3946828
- DOI: 10.1016/j.jpeds.2013.10.013
Kaposiform lymphangiomatosis: a distinct aggressive lymphatic anomaly
Abstract
Objective: To describe the clinical and imaging characteristics of a new lymphatic disorder with a unique histological pattern and poor prognosis.
Study design: An observational, retrospective study identified and characterized 20 patients with distinct lymphatic histopathology referred to the Vascular Anomalies Center at Boston Children's Hospital between 1995 and 2011.
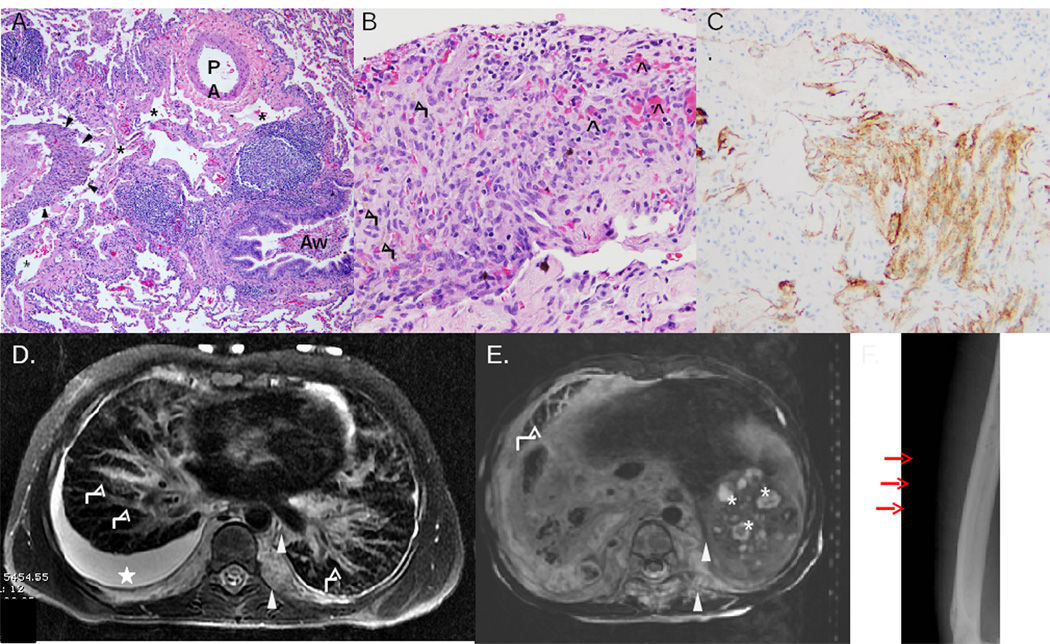
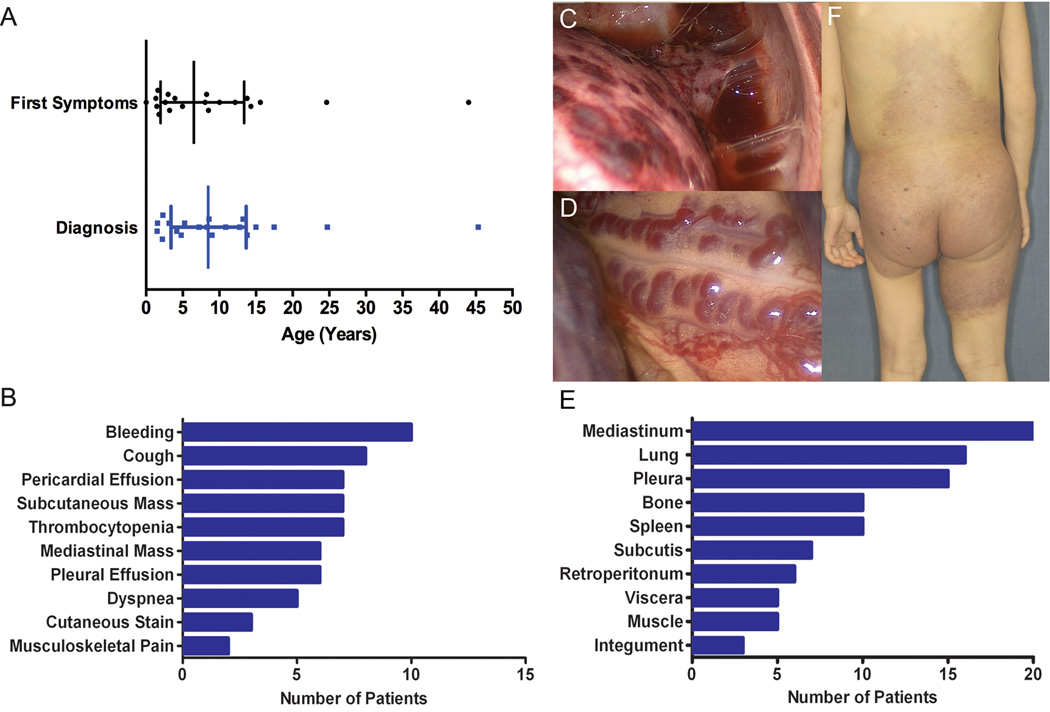
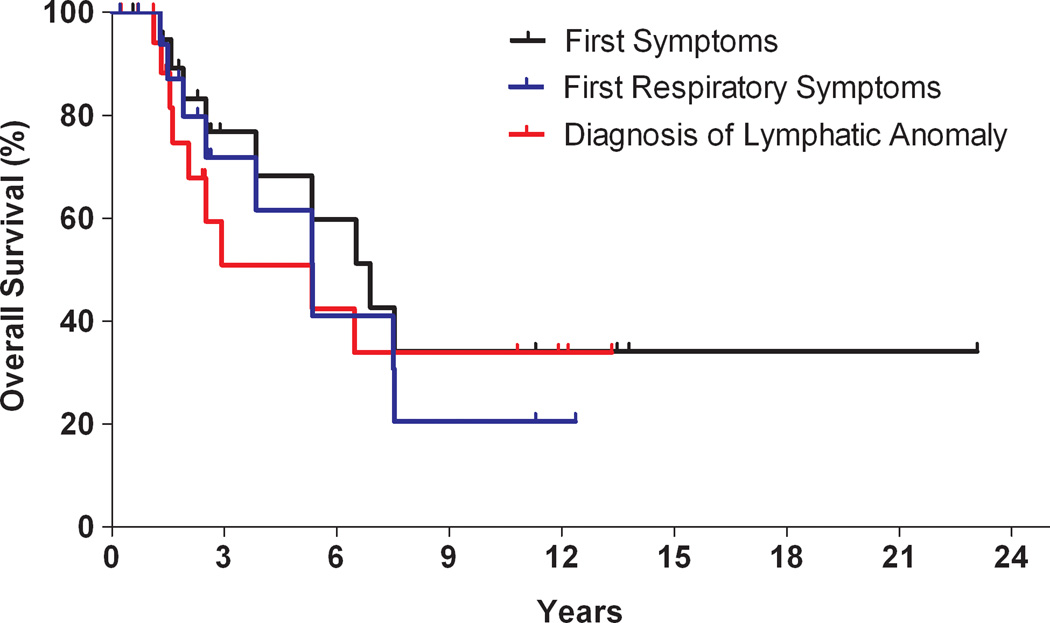
Results: The median age at onset was 6.5 years (range, birth to 44 years). Clinical and radiologic findings suggested a generalized process. The most common presentations were respiratory symptoms (50%), hemostatic abnormalities (50%), and an enlarging, palpable mass (35%). All patients had mediastinal involvement; 19 patients developed pericardial (70%) and/or pleural effusions (85%). Extrathoracic disease manifested in bone and spleen and less frequently in abdominal viscera, peritoneum, integument, and extremities. Despite aggressive procedural and medical therapies, the 5-year survival was 51% and the overall survival was 34%. Mean interval between diagnosis and death was 2.75 years (range, 1-6.5 years).
Conclusions: We describe a clinicopathologically distinct lymphatic anomaly. We propose the term kaposiform lymphangiomatosis (KLA) because of characteristic clusters or sheets of spindled lymphatic endothelial cells accompanying malformed lymphatic channels. The intrathoracic component is most commonly implicated in morbidity and mortality; however, extrathoracic disease is frequent, indicating that KLA is not restricted to pulmonary lymphatics. The mortality rate of KLA is high despite aggressive multimodal therapy.
Keywords: GLA; Generalized lymphatic anomaly; KHE; KLA; Kaposiform hemangioendothelioma; Kaposiform lymphangiomatosis; MRI; Magnetic resonance imaging.
Copyright © 2014 Mosby, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Detaille T, Joomye R, Barrea C, Clapuyt P, Boon LM, Clement de Clety S. Acute life-threatening presentation of unknown lymphatic malformation. Am J Emerg Med. 2010;28:1062 e1–1062 e3. - PubMed
-
- Greene AK, Burrows PE, Smith L, Mulliken JB. Periorbital lymphatic malformation: clinical course and management in 42 patients. Plast Reconstr Surg. 2005;115:22–30. - PubMed
-
- Hogeling M, Adams S, Law J, Wargon O. Lymphatic malformations: clinical course and management in 64 cases. Australas J Dermatol. 2011;52:186–190. - PubMed
-
- Faul JL, Berry GJ, Colby TV, Ruoss SJ, Walter MB, Rosen GD, et al. Thoracic lymphangiomas, lymphangiectasis, lymphangiomatosis, and lymphatic dysplasia syndrome. Am J Respir Crit Care Med. 2000;161:1037–1046. - PubMed
-
- Alvarez OA, Kjellin I, Zuppan CW. Thoracic lymphangiomatosis in a child. J Pediatr Hematol Oncol. 2004;26:136–141. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
