

Temporal and spatial evolution of somatic chromosomal alterations: a case-cohort study of Barrett's esophagus
- PMID: 24253313
- PMCID: PMC3904552
- DOI: 10.1158/1940-6207.CAPR-13-0289
Temporal and spatial evolution of somatic chromosomal alterations: a case-cohort study of Barrett's esophagus
Abstract
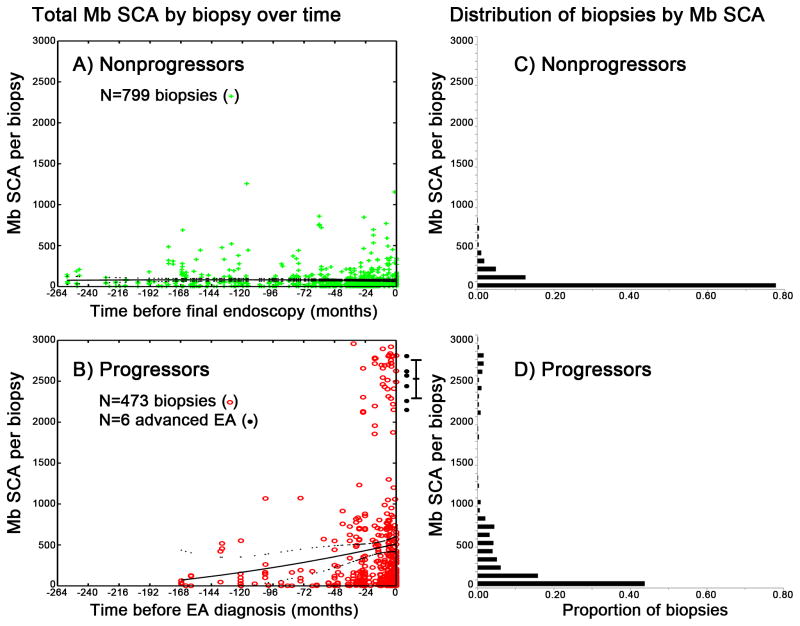
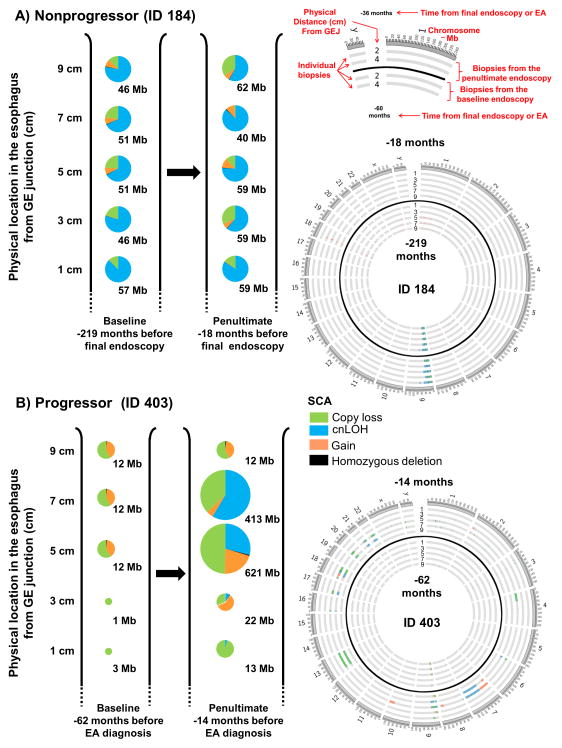
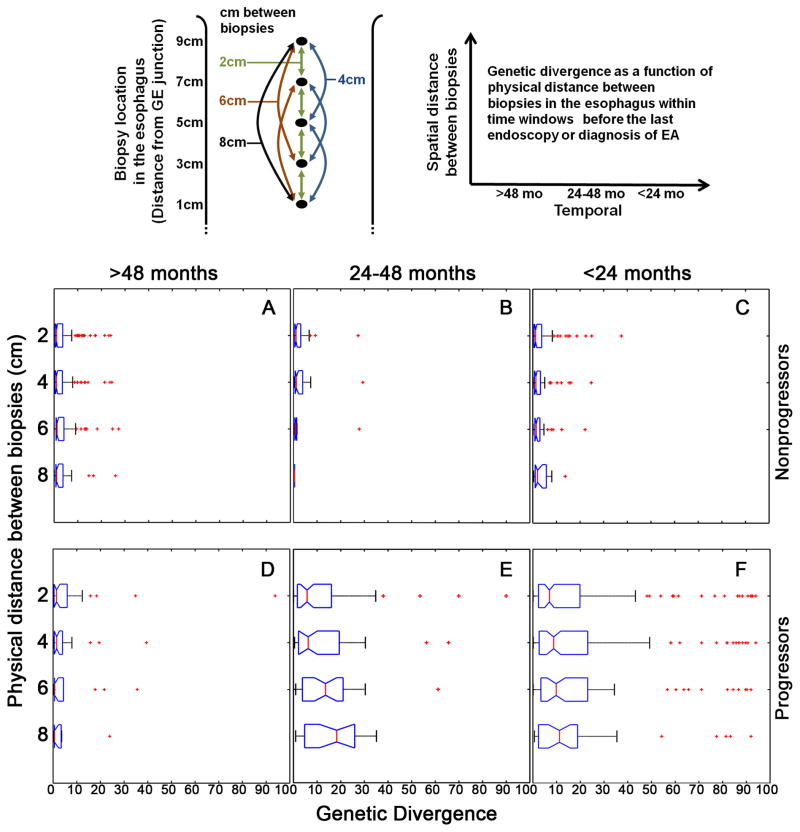
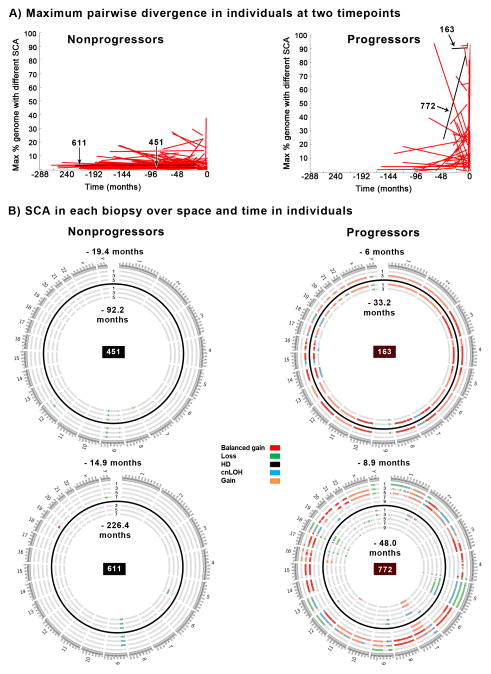
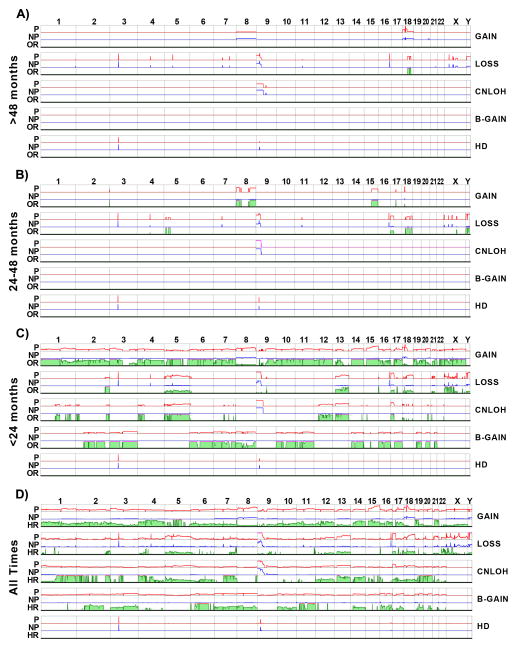
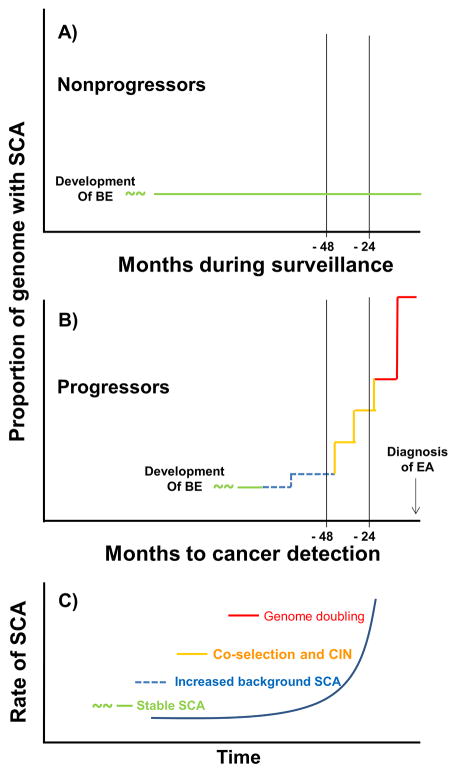
All cancers are believed to arise by dynamic, stochastic somatic genomic evolution with genome instability, generation of diversity, and selection of genomic alterations that underlie multistage progression to cancer. Advanced esophageal adenocarcinomas have high levels of somatic copy number alterations. Barrett's esophagus is a risk factor for developing esophageal adenocarcinoma, and somatic chromosomal alterations (SCA) are known to occur in Barrett's esophagus. The vast majority (∼95%) of individuals with Barrett's esophagus do not progress to esophageal adenocarcinoma during their lifetimes, but a small subset develop esophageal adenocarcinoma, many of which arise rapidly even in carefully monitored patients without visible endoscopic abnormalities at the index endoscopy. Using a well-designed, longitudinal case-cohort study, we characterized SCA as assessed by single-nucleotide polymorphism arrays over space and time in 79 "progressors" with Barrett's esophagus as they approach the diagnosis of cancer and 169 "nonprogressors" with Barrett's esophagus who did not progress to esophageal adenocarcinoma over more than 20,425 person-months of follow-up. The genomes of nonprogressors typically had small localized deletions involving fragile sites and 9p loss/copy neutral LOH that generate little genetic diversity and remained relatively stable over prolonged follow-up. As progressors approach the diagnosis of cancer, their genomes developed chromosome instability with initial gains and losses, genomic diversity, and selection of SCAs followed by catastrophic genome doublings. Our results support a model of differential disease dynamics in which nonprogressor genomes largely remain stable over prolonged periods, whereas progressor genomes evolve significantly increased SCA and diversity within four years of esophageal adenocarcinoma diagnosis, suggesting a window of opportunity for early detection.
©2013 AACR.
Conflict of interest statement
Figures
References
-
- Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005;97:142–6. - PubMed
-
- Dubecz A, Gall I, Solymosi N, Schweigert M, Peters JH, Feith M, et al. Temporal trends in long-term survival and cure rates in esophageal cancer: a SEER database analysis. J Thorac Oncol. 2012;7:443–7. - PubMed
-
- Li Z, Rice TW, Liu X, Goldblum JR, Williams SJ, Rybicki LA, et al. Intramucosal esophageal adenocarcinoma: primum non nocere. J Thorac Cardiovasc Surg. 2013;145:1519–24. 24 e1–3. - PubMed
-
- Rice TW, Zuccaro G, Jr, Adelstein DJ, Rybicki LA, Blackstone EH, Goldblum JR. Esophageal carcinoma: depth of tumor invasion is predictive of regional lymph node status. Ann Thorac Surg. 1998;65:787–92. - PubMed
-
- Prenzel KL, Holscher AH, Drebber U, Agavonova M, Gutschow CA, Bollschweiler E. Prognostic impact of nodal micrometastasis in early esophageal cancer. Eur J Surg Oncol. 2012;38:314–8. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
