

Assessment of concomitant paroxysmal atrial fibrillation ablation in mitral valve surgery patients based on continuous monitoring: does a different lesion set matter?
- PMID: 24254537
- PMCID: PMC3895064
- DOI: 10.1093/icvts/ivt461
Assessment of concomitant paroxysmal atrial fibrillation ablation in mitral valve surgery patients based on continuous monitoring: does a different lesion set matter?
Abstract
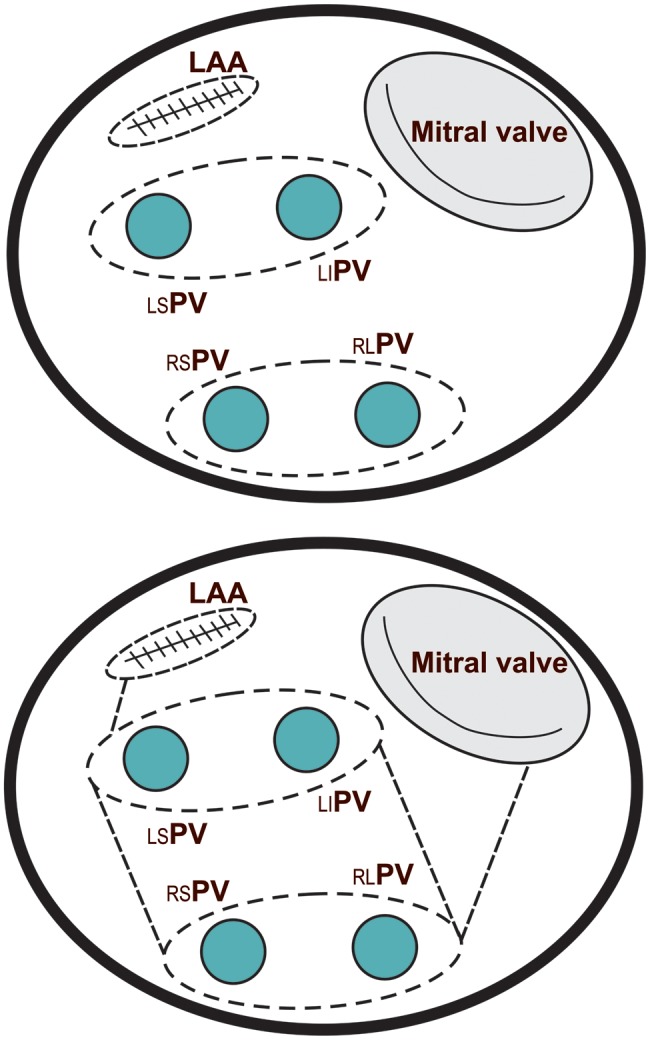
Objectives: The efficacy of concomitant ablation techniques in patients with paroxysmal atrial fibrillation (AF) undergoing mitral valve surgery remains under debate. The aim of this prospective, randomized, single-centre study was to compare pulmonary vein isolation (PVI) only versus a left atrial maze (LAM) procedure in patients with paroxysmal AF during mitral valve surgery.
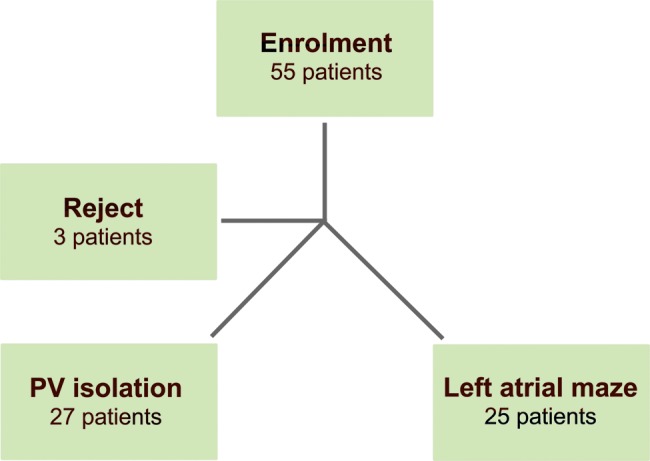
Methods: Between February 2009 and June 2011, 52 patients with a mean age of 54.2 (standard deviation 7.2 years) underwent mitral valve surgery and concomitant bipolar radiofrequency ablation for paroxysmal AF. Patients were randomized into the PVI group (n = 27) and the LAM group (n = 25). After surgery, an implantable loop recorder for continuous electrocardiography (ECG) monitoring was implanted. Patients with an AF burden (AF%) of <0.5% were considered AF free (responders). The mean follow-up was 18.6 months (standard deviation 2.1 months), and the patient' data were evaluated every 3 months.
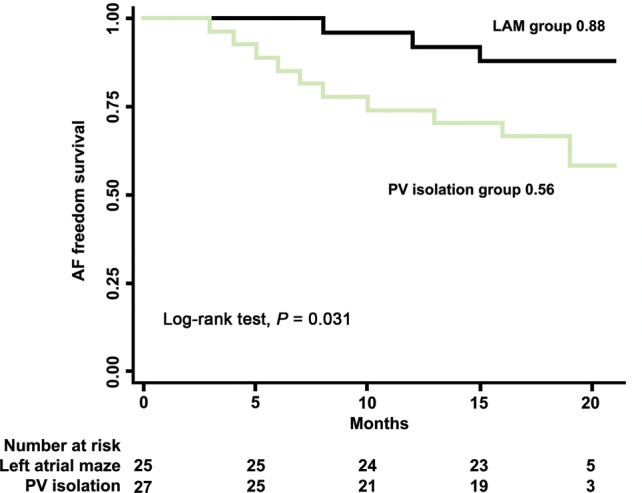
Results: All patients were alive at discharge. No procedure-related complications occurred for either the ablation or the loop recorder implantation. Mean aortic clamping and ablation times were significantly longer in the LAM group than in the PVI group. The incidence of early AF paroxysm recurrence was significantly higher in the PVI group than in the LAM group (62.9 vs 24.0%, P < 0.001). At 20 months after surgery, 15 (55.6%) of the 27 patients in the PVI group and 22 (88.0%) of the 25 patients in the LAM group had no documented atrial arrhythmias and were considered responders (AF burden <0.5%). The mean AF burden during all follow-up periods was significantly lower in the LAM group (23.6 ± 8.7%) than in the PVI group (6.8 ± 2.2%) (P < 0.001).
Conclusions: According to continuous ECG monitoring data, freedom from AF was significantly higher after the concomitant LAM procedure than after PVI in patients with paroxysmal AF who underwent mitral valve surgery.
Keywords: Atrial fibrillation; Continuous electrocardiography monitoring; Mitral valve surgery; Radiofrequency ablation.
Figures
Similar articles
-
Ablation for atrial fibrillation during mitral valve surgery: 1-year results through continuous subcutaneous monitoring.Interact Cardiovasc Thorac Surg. 2012 Jul;15(1):37-41. doi: 10.1093/icvts/ivs053. Epub 2012 Apr 18. Interact Cardiovasc Thorac Surg. 2012. PMID: 22514258 Free PMC article.
-
Circumferential pulmonary vein ablation with additional linear ablation results in an increased incidence of left atrial flutter compared with segmental pulmonary vein isolation as an initial approach to ablation of paroxysmal atrial fibrillation.Circ Arrhythm Electrophysiol. 2010 Jun;3(3):243-8. doi: 10.1161/CIRCEP.109.924878. Epub 2010 Mar 25. Circ Arrhythm Electrophysiol. 2010. PMID: 20339034 Clinical Trial.
-
Long-term results after the box pulmonary vein isolation procedure for chronic atrial fibrillation in mitral valve surgery.Ann Thorac Cardiovasc Surg. 2012;18(2):101-8. doi: 10.5761/atcs.oa.11.01733. Epub 2011 Nov 15. Ann Thorac Cardiovasc Surg. 2012. PMID: 22082812
-
How effective is microwave ablation for atrial fibrillation during concomitant cardiac surgery?Interact Cardiovasc Thorac Surg. 2012 Jul;15(1):122-7. doi: 10.1093/icvts/ivs137. Epub 2012 Apr 17. Interact Cardiovasc Thorac Surg. 2012. PMID: 22510269 Free PMC article. Review.
-
Clinical Implications of Ablation of Drivers for Atrial Fibrillation: A Systematic Review and Meta-Analysis.Circ Arrhythm Electrophysiol. 2018 May;11(5):e006119. doi: 10.1161/CIRCEP.117.006119. Circ Arrhythm Electrophysiol. 2018. PMID: 29743170 Free PMC article.
Cited by
-
Surgical treatment of atrial fibrillation in mitral valve surgery: a narrative review.J Thorac Dis. 2024 May 31;16(5):3461-3471. doi: 10.21037/jtd-23-1984. Epub 2024 May 28. J Thorac Dis. 2024. PMID: 38883625 Free PMC article. Review.
-
2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation.Europace. 2018 Jan 1;20(1):e1-e160. doi: 10.1093/europace/eux274. Europace. 2018. PMID: 29016840 Free PMC article. Review. No abstract available.
-
Preoperative Non-Invasive Mapping for Targeted Concomitant Surgical Ablation of Non-Paroxysmal Atrial Fibrillation (PreMap Study).J Clin Med. 2025 Jan 14;14(2):481. doi: 10.3390/jcm14020481. J Clin Med. 2025. PMID: 39860487 Free PMC article.
-
2023 KASNet Guidelines on Atrial Fibrillation Surgery.J Chest Surg. 2024 Jan 5;57(1):1-24. doi: 10.5090/jcs.23.127. Epub 2023 Nov 23. J Chest Surg. 2024. PMID: 37994091 Free PMC article. No abstract available.
-
Subcutaneouscardiac Rhythm Monitors: A Comprehensive Review.J Atr Fibrillation. 2021 Feb 28;13(5):2387. doi: 10.4022/jafib.2387. eCollection 2021 Feb-Mar. J Atr Fibrillation. 2021. PMID: 34950332 Free PMC article. Review.
References
-
- Kawaguchi A, Kosakai Y, Sasako Y, Eishi K, Nakano K, Kawashima Y. Risks and benefits of combined maze procedure for atrial fibrillation associated with organic heart disease. J Am Coll Cardiol. 1996;28:985–90. - PubMed
-
- Handa N, Schaff H, Morris J, Anderson B, Kopecky S, Enriquez-Sarano M. Outcome of valve repair and the Cox maze procedure for mitral regurgitation and associated atrial fibrillation. J Thorac Cardiovasc Surg. 1999;118:626–35. - PubMed
-
- Calkins H, Kuck K, Cappato R, Brugada J, Camm A, Chen S, et al. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Heart Rhythm. 2012;9:632–96. - PubMed
-
- Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339:659–66. - PubMed
-
- Marrouche NF, Dresing T, Cole C, Bash D, Saad E, Balaban K, et al. Circular mapping and ablation of the pulmonary vein for treatment of atrial fibrillation: impact of different catheter technologies. J Am Coll Cardiol. 2002;40:464–74. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
