

The effect of an EDTA-based chelation regimen on patients with diabetes mellitus and prior myocardial infarction in the Trial to Assess Chelation Therapy (TACT)
- PMID: 24254885
- PMCID: PMC4111470
- DOI: 10.1161/CIRCOUTCOMES.113.000663
The effect of an EDTA-based chelation regimen on patients with diabetes mellitus and prior myocardial infarction in the Trial to Assess Chelation Therapy (TACT)
Abstract
Background: The Trial to Assess Chelation Therapy (TACT) showed clinical benefit of an EDTA-based infusion regimen in patients aged ≥50 years with prior myocardial infarction. Diabetes mellitus before enrollment was a prespecified subgroup.
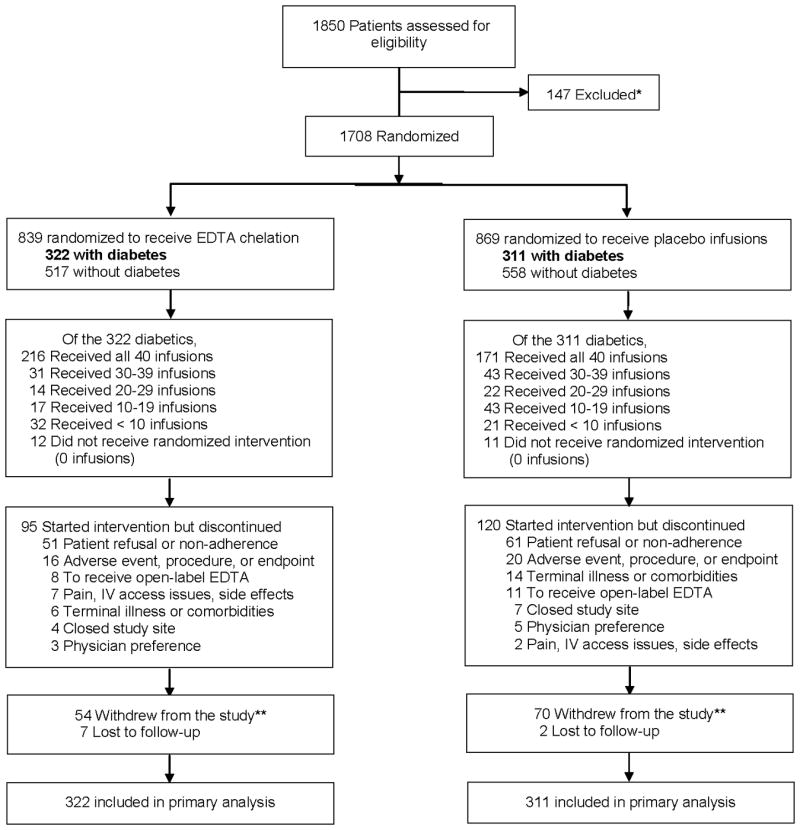
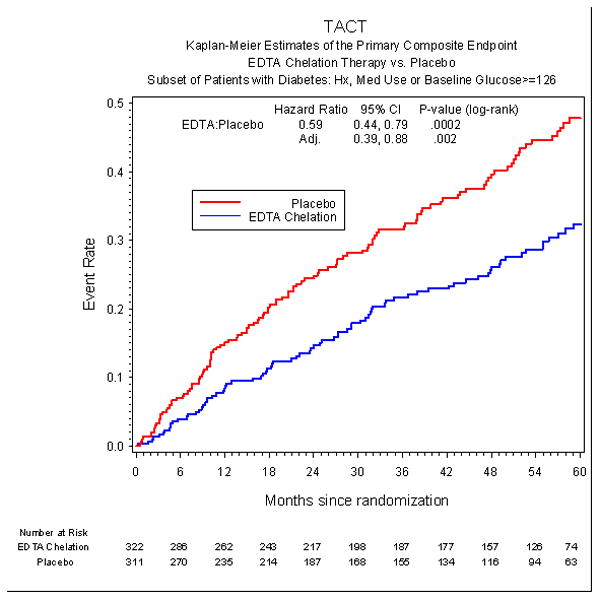
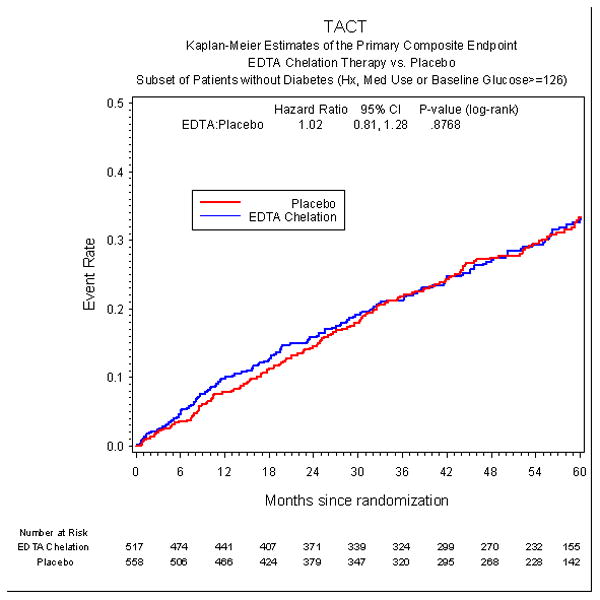
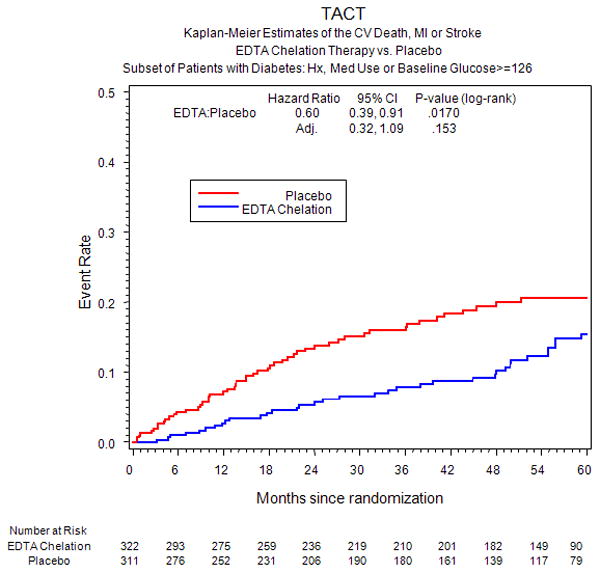
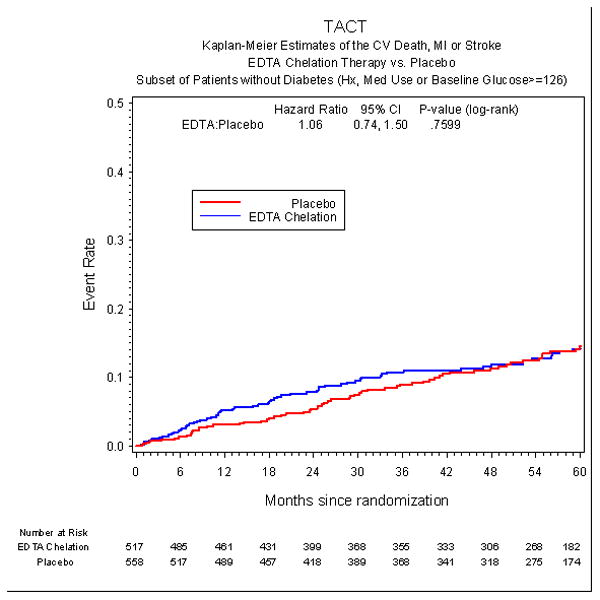
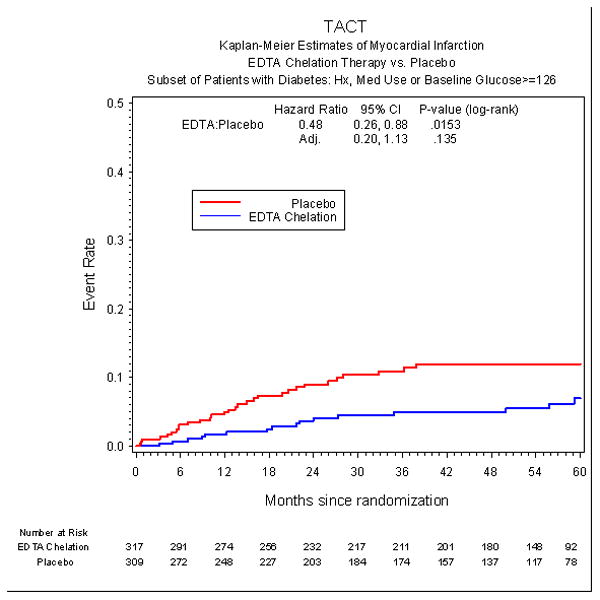
Methods and results: Patients received 40 infusions of EDTA chelation or placebo. A total of 633 (37%) patients had diabetes mellitus (322 EDTA and 311 placebo). EDTA reduced the primary end point (death, reinfarction, stroke, coronary revascularization, or hospitalization for angina; 25% versus 38%; hazard ratio, 0.59; 95% confidence interval [CI], 0.44-0.79; P<0.001) over 5 years. The result remained significant after Bonferroni adjustment for multiple subgroups (99.4% CI, 0.39-0.88; adjusted P=0.002). All-cause mortality was reduced by EDTA chelation (10% versus 16%; hazard ratio, 0.57; 95% CI, 0.36-0.88; P=0.011), as was the secondary end point (cardiovascular death, reinfarction, or stroke; 11% versus 17%; hazard ratio, 0.60; 95% CI, 0.39-0.91; P=0.017). However, after adjusting for multiple subgroups, those results were no longer significant. The number needed to treat to reduce 1 primary end point over 5 years was 6.5 (95% CI, 4.4-12.7). There was no reduction in events in non-diabetes mellitus (n=1075; P=0.877), resulting in a treatment by diabetes mellitus interaction (P=0.004).
Conclusions: Post-myocardial infarction patients with diabetes mellitus aged ≥50 demonstrated a marked reduction in cardiovascular events with EDTA chelation. These findings support efforts to replicate these findings and define the mechanisms of benefit. However, they do not constitute sufficient evidence to indicate the routine use of chelation therapy for all post-myocardial infarction patients with diabetes mellitus.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00044213.
Keywords: diabetes mellitus; myocardial infarction; secondary prevention.
Figures

Comment in
-
Are concerns about reliability in the trial to assess chelation therapy fair grounds for a hasty dismissal?: An alternative perspective.Circ Cardiovasc Qual Outcomes. 2014 Jan;7(1):5-7. doi: 10.1161/CIRCOUTCOMES.113.000714. Epub 2014 Jan 14. Circ Cardiovasc Qual Outcomes. 2014. PMID: 24425709 No abstract available.
References
-
- Clarke NE, Clarke CN, Mosher RE. The in vivo dissolution of metastatic calcium; an approach to atherosclerosis. Am J Med Sci. 1955;229:142–149. - PubMed
-
- Clarke CN, Clarke NE, Mosher RE. Treatment of angina pectoris with disodium ethylene diamine tetra acetic acid. Am J Med Sci. 1956;232:654–666. - PubMed
-
- Grier MT, Meyers DG. So much writing, so little science: a review of 37 years of literature on edetate sodium chelation therapy. Ann Pharmacother. 1993;27:1504–9. - PubMed
-
- National Institute of Health. EDTA Chelation Therapy for Coronary Artery Disease, RFA-AT-01004. http://grants.nih.gov/grants/guide/rfa-files/RFA-AT-01-004.html.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
