

Gene rearrangement study for minimal residual disease monitoring in children with acute lymphocytic leukemia
- PMID: 24255617
- PMCID: PMC3832314
- DOI: 10.5581/1516-8484.20130115
Gene rearrangement study for minimal residual disease monitoring in children with acute lymphocytic leukemia
Abstract
Objective: To detect markers for minimal residual disease monitoring based on conventional polymerase chain reaction for immunoglobulin, T-cell receptor rearrangements and the Sil-Tal1 deletion in patients with acute lymphocytic leukemia.
Methods: Fifty-nine children with acute lymphocytic leukemia from three institutions in Minas Gerais, Brazil, were prospectively studied. Clonal rearrangements were detected by polymerase chain reaction followed by homo/heteroduplex clonality analysis in DNA samples from diagnostic bone marrow. Follow-up samples were collected on Days 14 and 28-35 of the induction phase. The Kaplan-Meier and multivariate Cox methods were used for survival analysis.
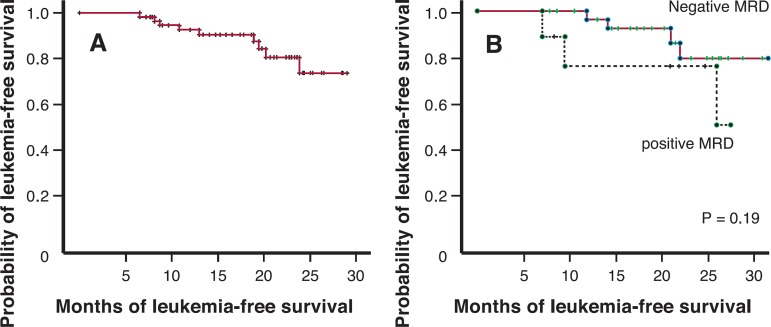
Results: Immunoglobulin/T-cell receptor rearrangements were not detected in 5/55 children screened (9.0%). For precursor-B acute lymphocytic leukemia, the most frequent rearrangement was IgH (72.7%), then TCRG (61.4%), and TCRD and IgK (47.7%); for T-acute lymphocytic leukemia, TCRG (80.0%), and TCRD and Sil-Tal deletion (20.0%) were the most common. Minimal residual disease was detected in 35% of the cases on Day 14 and in 22.5% on Day 28-35. Minimal residual disease on Day 28-35, T-acute lymphocytic leukemia, and leukocyte count above 50 x 10(9)/L at diagnosis were bad prognostic factors for leukemia-free survival in univariate analysis. Relapse risk for minimal residual disease positive relative to minimal residual disease negative children was 8.5 times higher (95% confidence interval: 1.02-70.7).
Conclusion: Immunoglobulin/T-cell receptor rearrangement frequencies were similar to those reported before. Minimal residual disease is an independent prognostic factor for leukemia-free survival, even when based on a non-quantitative technique, but longer follow-ups are needed.
Keywords: Gene rearrangement; Neoplasm, residual; Polymerase chain reaction; Precursor cell lymphoblastic leukemia-lymphoma.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interest
Figures
References
-
- Brandalise S, Odone V, Pereira W, Andrea M, Zanichelli M, Aranega V. Treatment results of three consecutive Brazilian cooperative childhood ALL protocols: GBTLI-80, GBTLI-82 and -85. ALL Brazilian Group. Leukemia. 1993;7(Suppl 2):S142–S145. - PubMed
-
- Brandalise SR, Pinheiro VR, Aguiar SS, Matsuda EI, Otubo R, Yunes JA, et al. Benefits of the intermittent use of 6-mercaptopurine and methotrexate in maintenance treatment for low-risk acute lymphoblastic leukemia in children: randomized trial from the Brazilian Childhood Cooperative Group-protocol ALL-99. J Clin Oncol. 2010;28(11):1911–1918. - PubMed
-
- Jacquy D, Delepaut B, Van Daele S, Vaerman JL, Zenebergh A, Brichard B, et al. A prospective study of minimal residual disease in childhood B-lineage acute lymphoblastic leukaemia: MRD level at the end of induction is a strong predictive factor of relapse. Br J Haematol. 1997;98(1):140–146. - PubMed
-
- Cavé H, van der Werff ten Bosch J, Suciu S, Guidal C, Waterkeyn C, Otten J, et al. Clinical significance of minimal residual disease in childhood acute lymphoblastic leukemia. European Organization for Research and Treatment of Cancer-Childhood Leukemia Cooperative Group. N Engl J Med. 1998;339(9):591–598. Comment in: N Engl J Med. 1998;339(9):6279; N Engl J Med. 1999;340(2):152-3; author reply 153-4; N Engl J Med. 1999; 340(2):153-4. - PubMed
-
- van Dongen JJ, Seriu T, Panzer-Grümayer ER, Biondi A, Pongers-Willemse MJ, Corral L, et al. Prognostic value of minimal residual disease in acute lymphoblastic leukaemia in childhood. Lancet. 1998;352(9142):1731–1738. Comment in: Lancet. 1999; 353(9154):752-3. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous