Efficacy of an enuresis alarm, desmopressin, and combination therapy in the treatment of saudi children with primary monosymptomatic nocturnal enuresis
- PMID: 24255762
- PMCID: PMC3830973
- DOI: 10.4111/kju.2013.54.11.783
Efficacy of an enuresis alarm, desmopressin, and combination therapy in the treatment of saudi children with primary monosymptomatic nocturnal enuresis
Abstract
Purpose: We evaluated and compared the effectiveness of an enuresis alarm, desmopressin medication, and their combination in the treatment of Saudi children with primary monosymptomatic nocturnal enuresis (PMNE).
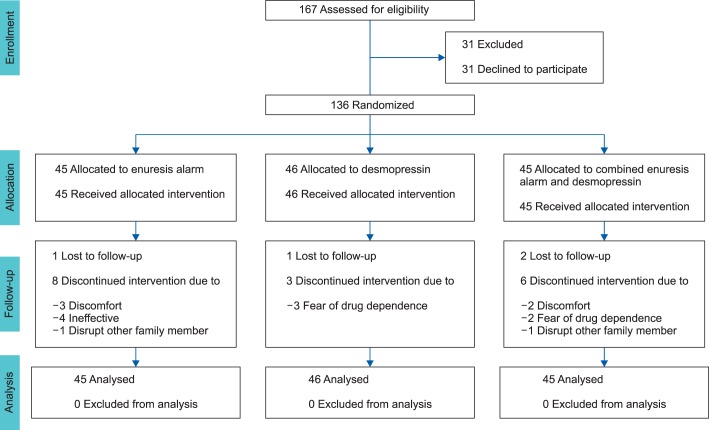
Materials and methods: A total of 136 children with PMNE were randomly assigned to receive an enuresis alarm alone (EA group, n=45), desmopressin alone (D group, n=46), or a combination of both (EA/D group, n=45). Patients were followed weekly during treatment and for 12 weeks after treatment withdrawal.
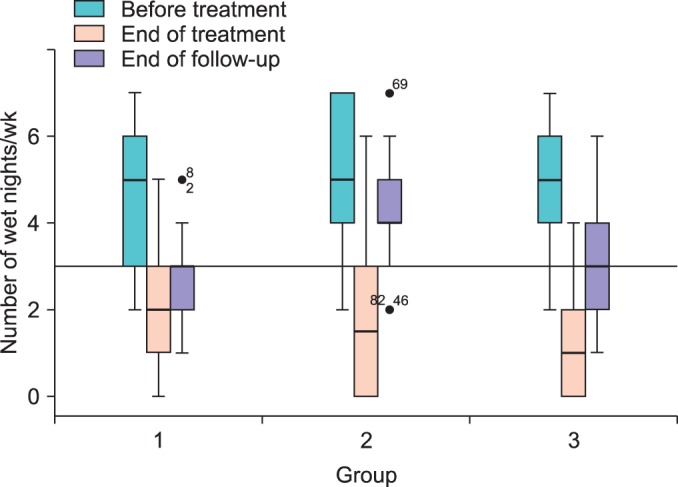
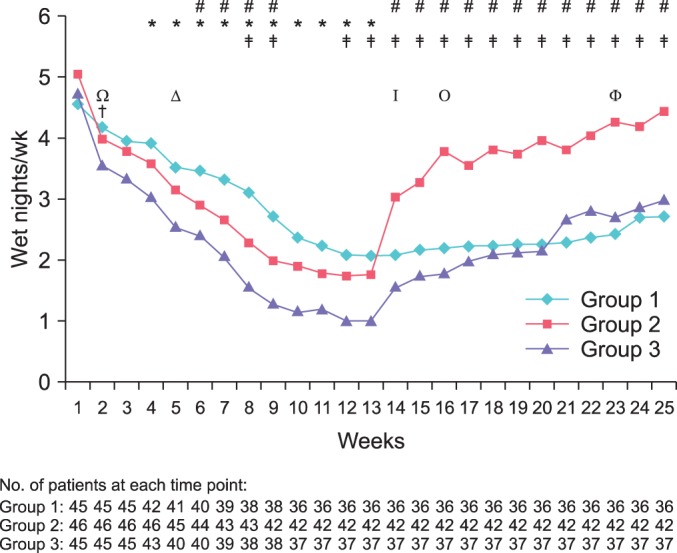
Results: During treatment, wetting frequencies were significantly reduced in all groups and remained significantly lower than pretreatment values until the end of follow-up. In the D and EA/D groups, an immediate reduction in wetting frequencies was observed, whereas a longer time was required to reach a significant reduction in the EA group. The full and partial response rates were 13.3% and 37.8% in the EA group, 26.1% and 43.5% in the D group, and 40.0% and 33.3% in the EA/D group. A significant difference was observed only between the EA and EA/D groups (p=0.025). Relapse rates were higher in the D group (66.6%) than in the EA (16.6%) and EA/D (33.3%) groups. A significant difference was observed between the D and EA groups only (p=0.019).
Conclusions: Desmopressin, an enuresis alarm, and combined therapy are effective in the treatment of Saudi children with PMNE. Desmopressin produced an immediate effect but relapses were common. The enuresis alarm provided gradual effects that persisted posttreatment. The combined therapy was superior to the alarm in achieving an immediate response; however, its effect was not better than that of the alarm long term.
Keywords: Combined modality therapy; Nocturnal enuresis; Treatment efficacy.
Conflict of interest statement
The authors have nothing to disclose.
Figures
Similar articles
-
Efficacy of desmopressin combined with alarm therapy for monosymptomatic nocturnal enuresis.J Urol. 2001 Dec;166(6):2456-8. J Urol. 2001. PMID: 11696811 Clinical Trial.
-
Comparison of long-term efficacy of desmopressin lyophilisate and enuretic alarm for monosymptomatic enuresis and assessment of predictive factors for success: a randomized prospective trial.J Urol. 2015 Feb;193(2):655-61. doi: 10.1016/j.juro.2014.08.088. Epub 2014 Aug 23. J Urol. 2015. PMID: 25158273 Clinical Trial.
-
The efficacy of the addition of short-term desmopressin to alarm therapy in the treatment of primary nocturnal enuresis.Int Urol Nephrol. 2008;40(3):583-6. doi: 10.1007/s11255-008-9355-6. Epub 2008 Mar 5. Int Urol Nephrol. 2008. PMID: 18320340 Clinical Trial.
-
Advances in the management of primary monosymptomatic nocturnal enuresis in children.Paediatr Int Child Health. 2016 Feb;36(1):7-14. doi: 10.1179/2046905515Y.0000000023. Epub 2015 May 2. Paediatr Int Child Health. 2016. PMID: 25936863 Review.
-
Therapeutic options in childhood nocturnal enuresis.Minerva Urol Nefrol. 2007 Jun;59(2):199-205. Minerva Urol Nefrol. 2007. PMID: 17571056 Review.
Cited by
-
Alarm interventions for nocturnal enuresis in children.Cochrane Database Syst Rev. 2020 May 4;5(5):CD002911. doi: 10.1002/14651858.CD002911.pub3. Cochrane Database Syst Rev. 2020. PMID: 32364251 Free PMC article.
-
Monosymptomatic nocturnal enuresis in pediatric patients: multidisciplinary assessment and effects of therapeutic intervention.Pediatr Nephrol. 2017 May;32(5):843-851. doi: 10.1007/s00467-016-3510-6. Epub 2016 Dec 17. Pediatr Nephrol. 2017. PMID: 27988804 Clinical Trial.
-
Desmopressin plus anticholinergic agent in the treatment of nocturnal enuresis: A meta-analysis.Exp Ther Med. 2017 Oct;14(4):2875-2884. doi: 10.3892/etm.2017.4897. Epub 2017 Aug 7. Exp Ther Med. 2017. PMID: 28966673 Free PMC article.
-
Monosymptomatic Nocturnal Enuresis Treatment Using Alarm-Therapy and Desmopressin: A Meta-analysis Approach.Med Arch. 2021 Dec;75(6):431-435. doi: 10.5455/medarh.2021.75.431-435. Med Arch. 2021. PMID: 35169370 Free PMC article.
-
The impact of adding low-dose oral desmopressin therapy to tamsulosin therapy for treatment of nocturia owing to benign prostatic hyperplasia.World J Urol. 2015 May;33(5):649-57. doi: 10.1007/s00345-014-1378-2. Epub 2014 Aug 20. World J Urol. 2015. PMID: 25138579 Clinical Trial.
References
-
- Yamamoto LG, Inaba AS, Okamoto JK, Patrinos ME, Yamashiroya VK, editors. Case based pediatrics for medical students and residents [monograph on the Internet] Honolulu: Department of Pediatrics, University of Hawaii John A Burns School of Medicine; c2004. [cited 2010 May 28]. Enuresis; pp. 5–28. Available from: http://www.hawaii.edu/medicine/pediatrics/pedtext/
-
- Butler RJ, Golding J, Northstone K ALSPAC Study Team. Nocturnal enuresis at 7.5 years old: prevalence and analysis of clinical signs. BJU Int. 2005;96:404–410. - PubMed
-
- Ozden C, Ozdal OL, Altinova S, Oguzulgen I, Urgancioglu G, Memis A. Prevalence and associated factors of enuresis in Turkish children. Int Braz J Urol. 2007;33:216–222. - PubMed
-
- Butler RJ, Heron J. The prevalence of infrequent bedwetting and nocturnal enuresis in childhood: A large British cohort. Scand J Urol Nephrol. 2008;42:257–264. - PubMed
-
- Butler RJ. Impact of nocturnal enuresis on children and young people. Scand J Urol Nephrol. 2001;35:169–176. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical