

Tracheobronchopathia osteochondroplastica: a case report and literature review
- PMID: 24255788
- PMCID: PMC3815732
- DOI: 10.3978/j.issn.2072-1439.2013.08.64
Tracheobronchopathia osteochondroplastica: a case report and literature review
Abstract
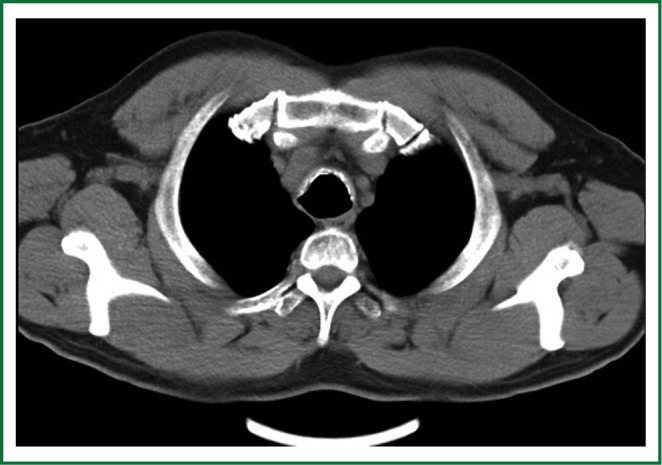
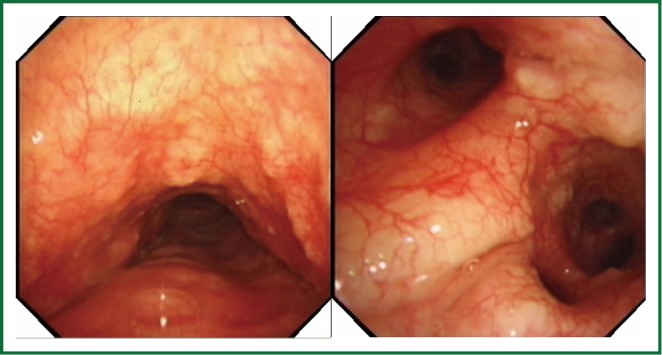
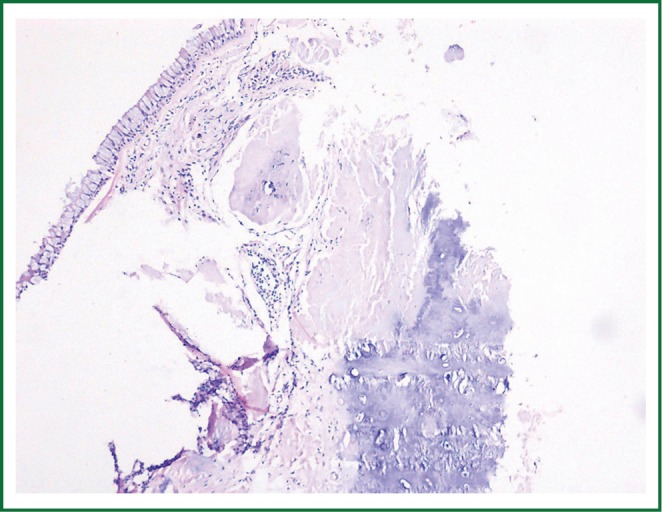
Tracheobronchopathia osteochondroplastica (TO) was diagnosed in a 52-year-old male with prolonged dry cough. Computerized tomography (CT) demonstrated that there were multiple calcified nodules in the anterolateral wall of trachea, sparing the posterior tracheal membrane. Fiberoptic bronchoscopy (FOB) showed that submucosal nodules protruded into the airway lumen. Histopathological exam found ossification and cartilage in the submucosa. TO is a scarce benign disorder, characterized by submucosal bony and cartilaginous nodules. The clinical manifestation is undistinguished and treatment is symptomatically dependent. FOB is a definitive diagnostic procedure. The characteristics of FOB finding are described as beaded, spiculate, rock garden, or cobble-stoned like nodules, which projected into the tracheobronchus lumen, sparing the posterior wall. Histopathological exam might re-confirm the diagnosis, finding ossification and cartilage in the submucosa of airway. Awareness of TO is significantly important, especially in chronic cough patients with special CT image, and FOB should be performed to confirm the diagnosis.
Keywords: Tracheobronchopathia osteochondroplastica (TO); cough; fiberoptic bronchoscopy (FOB).
Figures
References
-
- Wilks S.Ossific deposits on the larynx, trachea and bronchi. Trans Pathol Soc Lond 1857;8:88
-
- Lundgren R, Stjernberg NL. Tracheobronchopathia osteochondroplastica. A clinical bronchoscopic and spirometric study. Chest 1981;80:706-9 - PubMed
-
- Baran A, Güngör S, Unver E, et al. Tracheobronchopathia osteochondroplastica: a case report. Tuberk Toraks 2004;52:183-5 - PubMed
-
- Pounder DJ, Pieterse AS. Tracheopathia osteoplastica: a study of the minimal lesion. J Pathol 1982;138:235-9 - PubMed
-
- Abu-Hijleh M, Lee D, Braman SS. Tracheobronchopathia osteochondroplastica: a rare large airway disorder. Lung 2008;186:353-9 - PubMed
Publication types
LinkOut - more resources
Full Text Sources