

Improvement of long-term outcomes in pancreatic cancer and its associated factors within the gemcitabine era: a collaborative retrospective multicenter clinical review of 1,082 patients
- PMID: 24256464
- PMCID: PMC3766232
- DOI: 10.1186/1471-230X-13-134
Improvement of long-term outcomes in pancreatic cancer and its associated factors within the gemcitabine era: a collaborative retrospective multicenter clinical review of 1,082 patients
Abstract
Background: Although the outcomes of pancreatic cancer have been improved by gemcitabine, the changes in its characteristics and long-term outcomes within the gemcitabine era remain unclear. This study was conducted to identify clinical characteristics of pancreatic cancer patients within the gemcitabine era.
Methods: A retrospective chart review was performed at 10 centers for 1,248 consecutive patients who were ever considered to have a diagnosis of pancreatic cancer between 2001 and 2010. Data collected included demographics, diagnosis date, clinical stage, treatment, and outcome 1,082 patients met the inclusion criteria and were analyzed further. The chi-square test, Student's t-test, and Mann-Whitney U-test were used for statistical analysis. Outcomes were analyzed using the Kaplan-Meier method and Cox proportional hazards regression. Differences in survival analyses were determined using the log-rank test.
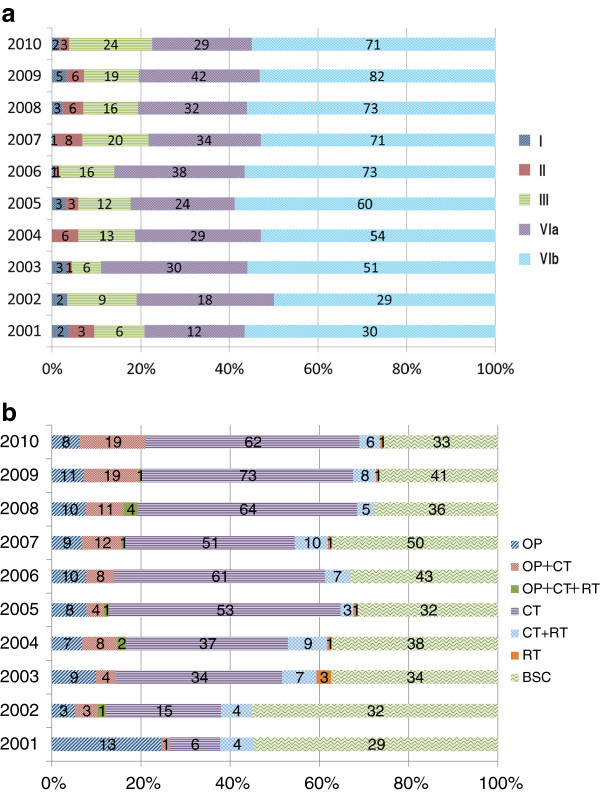
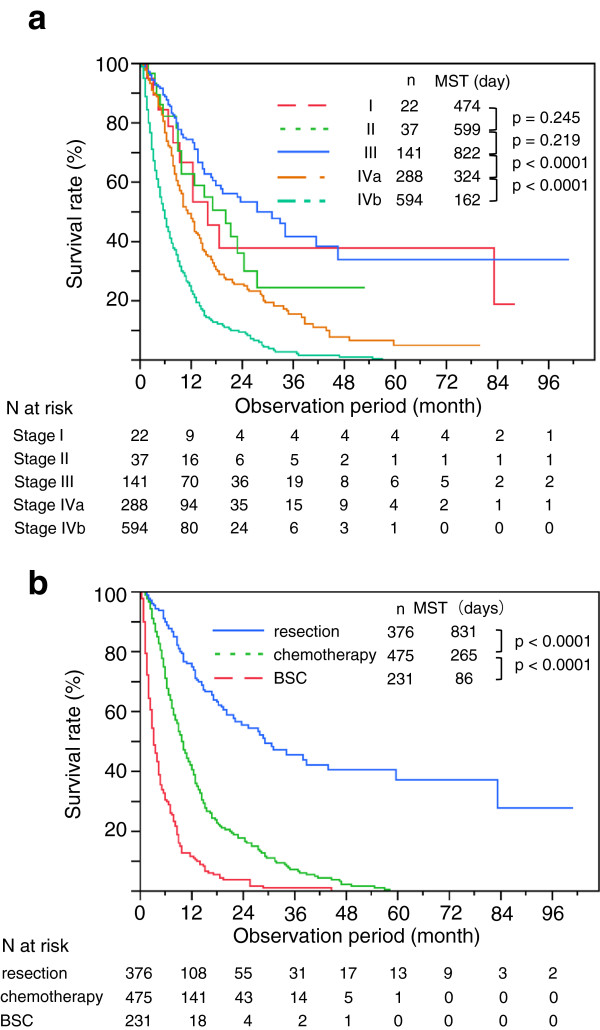
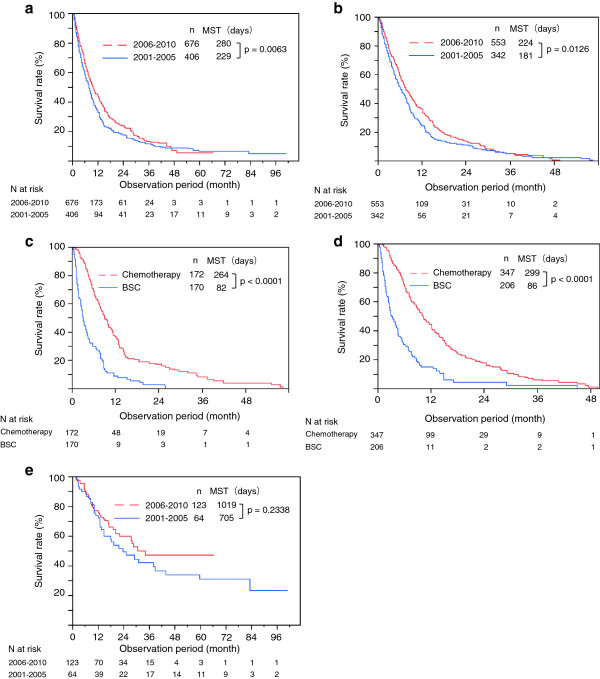
Results: The distribution of clinical stages was: I, 2.2% II, 3.4% III, 13% IVa, 27% and IVb, 55%. Chemotherapy alone was administered to 42% of patients and 17% underwent resection. The 1-, 3-, and 5-year survival rates were 39%, 13%, and 6.9%, respectively. The median survival time was 257 days, but differed considerably among treatments and clinical stages. Demographics, distribution of clinical stage, and cause of death did not differ between groups A (2001-2005, n=406) and B (2006-2010, n=676). However, group B included more patients who underwent chemotherapy (P<0.0001) and fewer treated with best supportive care (P=0.0004), mirroring improvements in this group's long-term outcomes (P=0.0063). Finally, factors associated with long-term outcomes derived from multivariate analysis were clinical stage (P<0.0001), location of the tumor (P=0.0294) and treatments (surgery, chemotherapy) (<0.0001).
Conclusions: Long-term outcomes in pancreatic cancer has improved even within the gemcitabine era, suggesting the importance of offering chemotherapy to patients previously only considered for best supportive care. Most patients are still diagnosed at an advanced stage, making clinical strategy development for diagnosing pancreatic cancer at earlier stages essential.
Figures
References
-
- Tanaka M. Japan Pancreas Society. Pancreatic Cancer Registry Report 2007 (in Japanese with English Abstract) Suizou. 2007;22:e1–e94.
-
- Isaji S, Kawarada Y. Evaluation of classification of pancreatic cancer by the Japan Pancreas Society and Union Internationale Contre le Cancer and proposal for a new international classification (in Japanese with English Abstract) Nihon Geka Gakkai Zasshi. 2000;101:205–211. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
