

High rates of tuberculosis in patients accessing HAART in rural South Africa
- PMID: 24256629
- PMCID: PMC3943690
- DOI: 10.1097/QAI.0000000000000060
High rates of tuberculosis in patients accessing HAART in rural South Africa
Abstract
Background: The challenge of early tuberculosis (TB) infection among rural patients accessing highly active antiretroviral therapy (HAART) in a resource-limited setting with high HIV and TB burden has not been fully quantified.
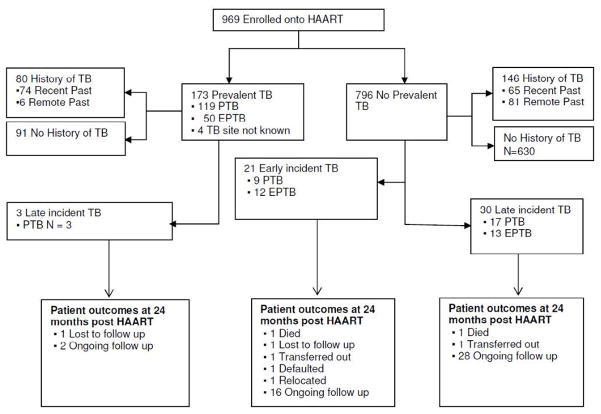
Methods: This is a retrospective study nested within a prospective study of 969 patients consecutively initiated onto HAART at the CAPRISA AIDS Treatment programme in rural KwaZulu-Natal between January 2007 and December 2010. Patients were screened for clinical symptoms consistent with TB using a standardized checklist, and routine clinical investigations that included sputum microscopy and chest x-ray diagnosis.
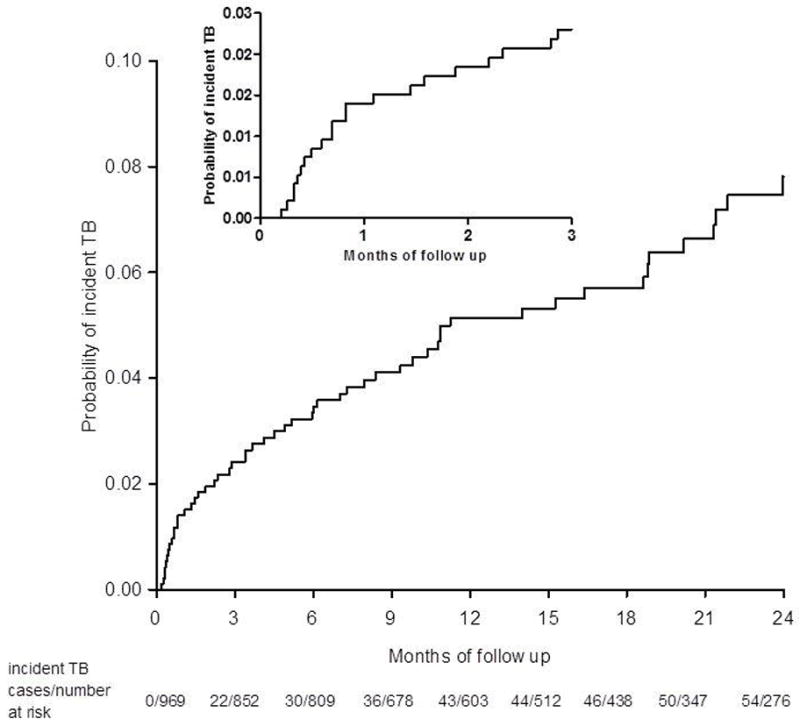
Results: Of 969 HIV-infected patients initiated on HAART, 173 [17.9%; 95% confidence interval (CI): 15.5 to 20.4] had active TB at HAART initiation. TB incidence rates were 3-fold higher in the first 3 months (early incident TB) after HAART initiation [11.5/100 person-years (py); 95% CI: 7.1 to 17.5] compared with 4-24 months (late incident TB) post-HAART initiation (3.2/100 py; 95% CI: 2.2 to 4.5; incidence rate ratio: 3.6; 95% CI: 2.0 to 6.4; P < 0.001). Immune status of patients at HAART initiation did not impact TB incidence rates in patients with CD4 counts of <50 (5.3/100) and >200 (4.9/100 py; P = 0.81) cells per cubic millimeter. CD4 count gains achieved 12 months post-HAART initiation were significantly different in patients with early incident TB versus late incident TB; P = 0.03.
Conclusions: Rural HIV treatment programmes in TB-endemic settings experience high rates of TB irrespective of immunologic status of patients at HAART initiation, or duration on HAART.
Conflict of interest statement
Conflicts of Interest
All authors declare no conflicts of interest.
Figures
References
-
- WHO. Global tuberculosis control - epidemiology, strategy, financing. WHO Report 2009. Geneva, Switzerland: 2009.
-
- W.H.O. Global Tuberculosis Control 2011. Geneva, Switzerland: 2011. http://www.who.int/tb/publications/global_report/2011/gtbr11_full.pdf.
-
- Barnighausen T, Tanser F, Gqwede Z, Mbizana C, Herbst K, Newell ML. High HIV incidence in a community with high HIV prevalence in rural South Africa: findings from a prospective population-based study. AIDS. 2008 Jan 2;22(1):139–144. - PubMed
-
- HST. [Accessed December 2010.];Reported cases of TB (all types) (per 100 000) http://www.hst.org.za/healthstats/16/data.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
