

Fibrinolysis greater than 3% is the critical value for initiation of antifibrinolytic therapy
- PMID: 24256667
- PMCID: PMC4072127
- DOI: 10.1097/TA.0b013e3182aa9c9f
Fibrinolysis greater than 3% is the critical value for initiation of antifibrinolytic therapy
Abstract
Background: The acute coagulopathy of trauma is present in up to one third of patients by the time of admission, and the recent CRASH-2 and MATTERs trials have focused worldwide attention on hyperfibrinolysis as a component of acute coagulopathy of trauma. Thromboelastography (TEG) is a powerful tool for analyzing fibrinolyis, but a clinically relevant threshold for defining hyperfibrinolysis has yet to be determined. Recent data suggest that the accepted normal upper bound of 7.5% for 30-minute fibrinolysis (LY30) by TEG is inappropriate in severe trauma, as the risk of death rises at much lower levels of clot lysis. We wished to determine the validity of this hypothesis and establish a threshold value to treat fibrinolysis, based on prediction of massive transfusion requirement and risk of mortality.
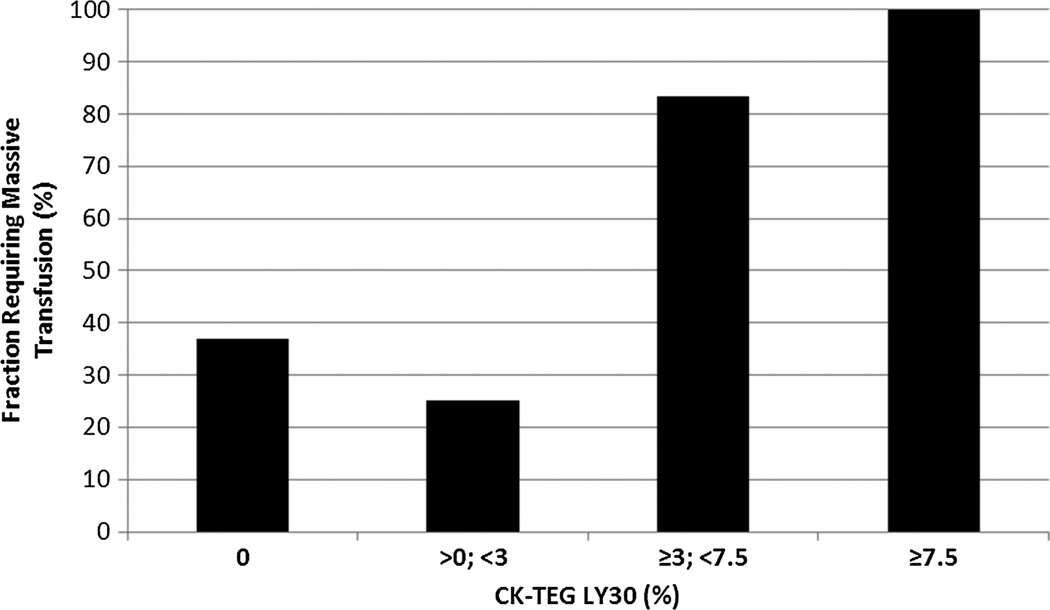
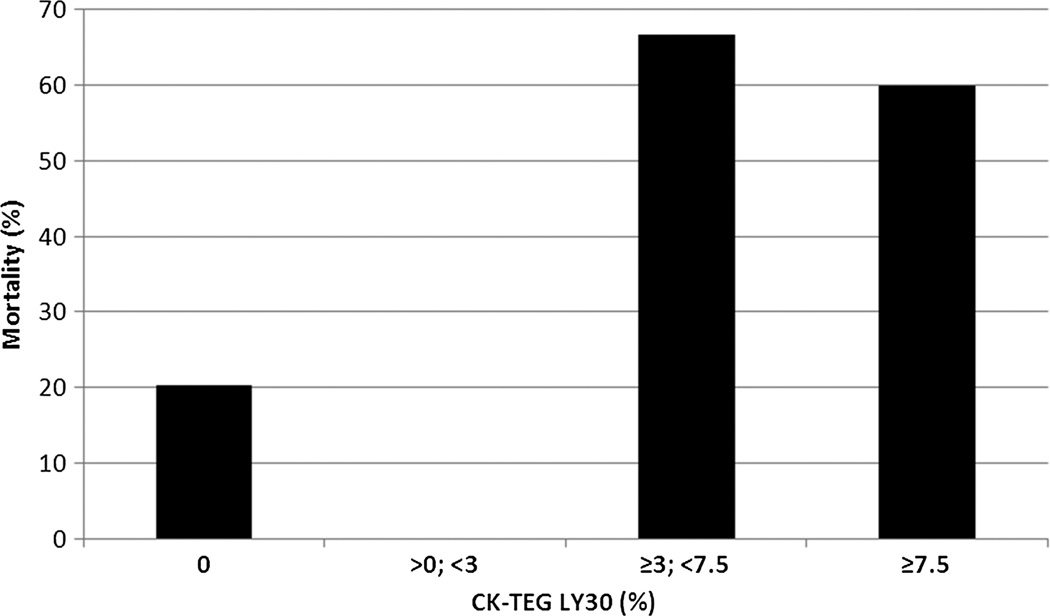
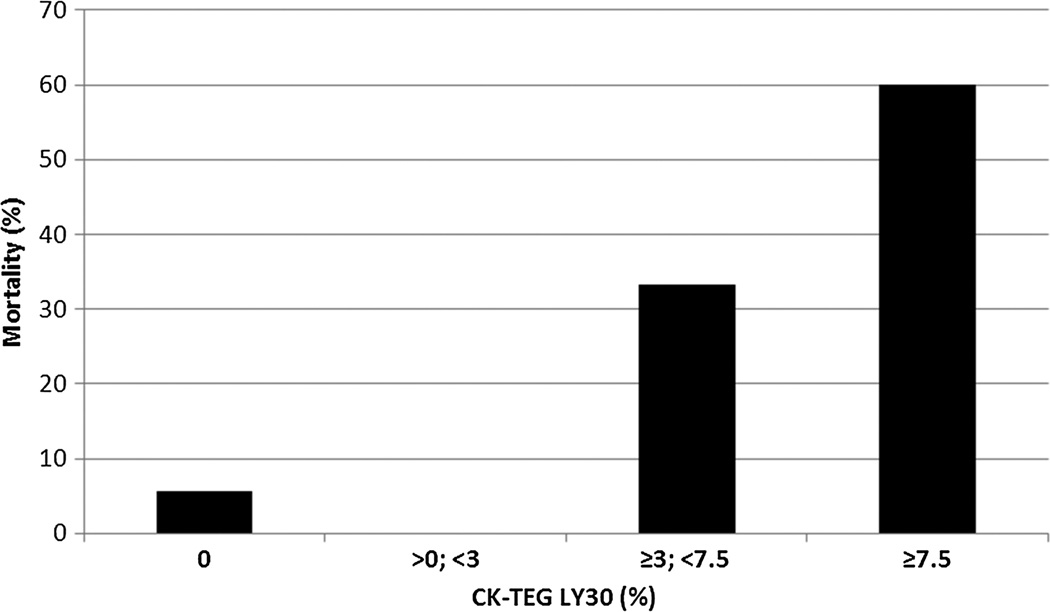
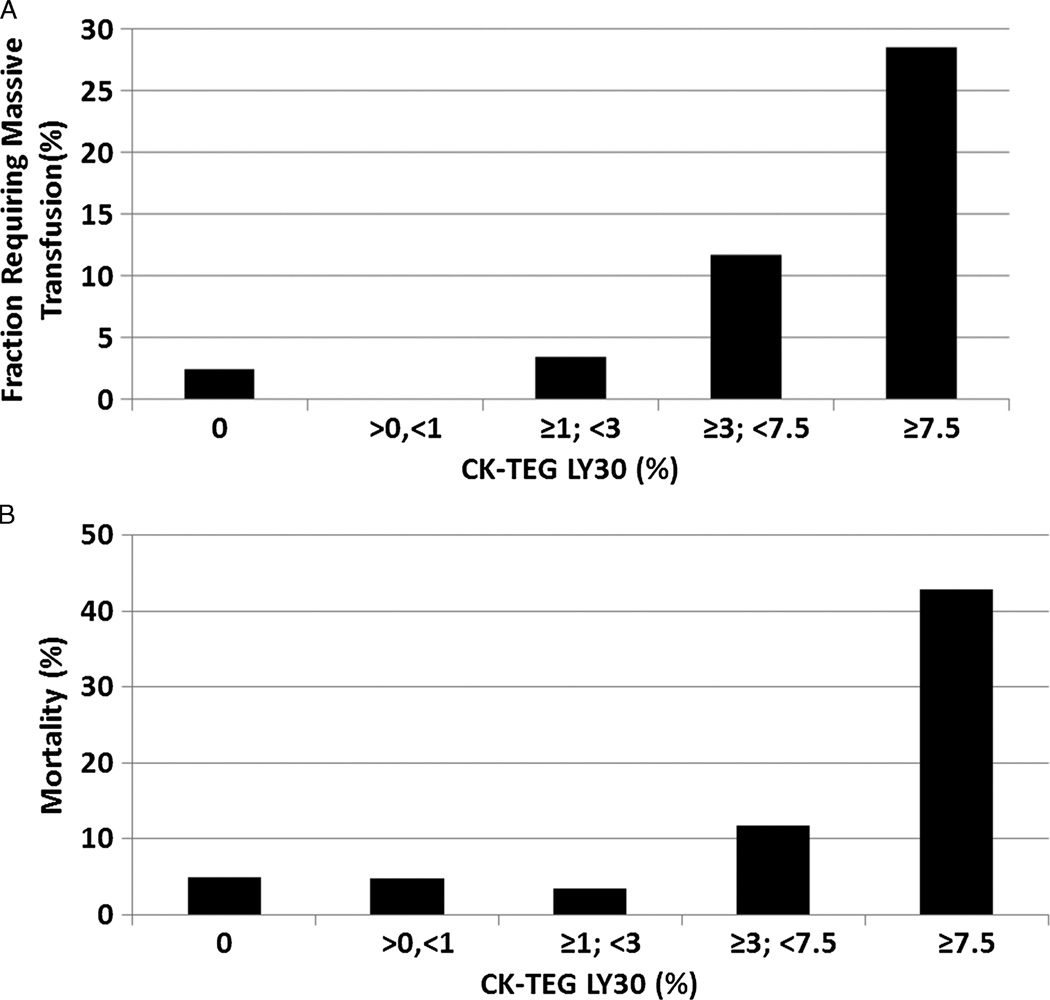
Methods: Patients with uncontrolled hemorrhage, meeting the massive transfusion protocol (MTP) criteria at admission (n = 73), represent the most severely injured trauma population at our center (median Injury Severity Score [ISS], 30; interquartile range, 20-38). Citrated kaolin TEG was performed at admission blood samples from this population, stratified by LY30, and evaluated for transfusion requirement and 28-day mortality. The same analysis was conducted on available field blood samples from all non-MTP trauma patients (n = 216) in the same period. These represent the general trauma population.
Results: Within the MTP-activating population, the cohort of patients with LY30 of 3% or greater was shown to be at much higher risk for requiring a massive transfusion (90.9% vs. 30.5%, p = 0.0008) and dying of hemorrhage (45.5% vs. 4.8%, p = 0.0014) than those with LY30 less than 3%. Similar trends were seen in the general trauma population.
Conclusion: LY30 of 3% or greater defines clinically relevant hyperfibrinolysis and strongly predicts the requirement for massive transfusion and an increased risk of mortality in trauma patients presenting with uncontrolled hemorrhage. This threshold value for LY30 represents a critical indication for the treatment of fibrinolysis.
Level of evidence: Prognostic study, level III.
Figures
References
-
- Armand R, Hess JR. Treating coagulopathy in trauma patients. Transfus Med Rev. 2003;17(3):223–231. - PubMed
-
- Brohi K, Cohen MJ, Davenport RA. Acute coagulopathy of trauma: mechanism, identification and effect. Curr Opin Crit Care. 2007;13(6):680–685. - PubMed
-
- Cohen MJ. Towards hemostatic resuscitation: the changing understanding of acute traumatic biology, massive bleeding, and damage-control resuscitation. Surg Clin North Am. 2012;92(4):877–891. viii. - PubMed
-
- Ganter MT, Pittet JF. New insights into acute coagulopathy in trauma patients. Best Pract Res Clin Anaesthesiol. 2010;24(1):15–25. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
