

Physician-assessed and patient-reported outcome measures in chemotherapy-induced sensory peripheral neurotoxicity: two sides of the same coin
- PMID: 24256846
- PMCID: PMC3868322
- DOI: 10.1093/annonc/mdt409
Physician-assessed and patient-reported outcome measures in chemotherapy-induced sensory peripheral neurotoxicity: two sides of the same coin
Abstract
Background: The different perception and assessment of chemotherapy-induced peripheral neurotoxicity (CIPN) between healthcare providers and patients has not yet been fully addressed, although these two approaches might eventually lead to inconsistent, possibly conflicting interpretation, especially regarding sensory impairment.
Patients and methods: A cohort of 281 subjects with stable CIPN was evaluated with the National Cancer Institute-Common Toxicity Criteria (NCI-CTC v. 2.0) sensory scale, the clinical Total Neuropathy Score (TNSc©), the modified Inflammatory Neuropathy Cause and Treatment (INCAT) sensory sumscore (mISS) and the European Organization for Research and Treatment of Cancer CIPN specific self-report questionnaire (EORTC QOL-CIPN20).
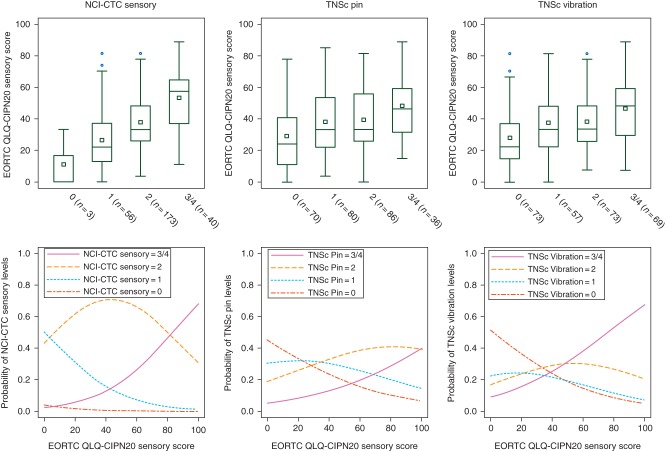
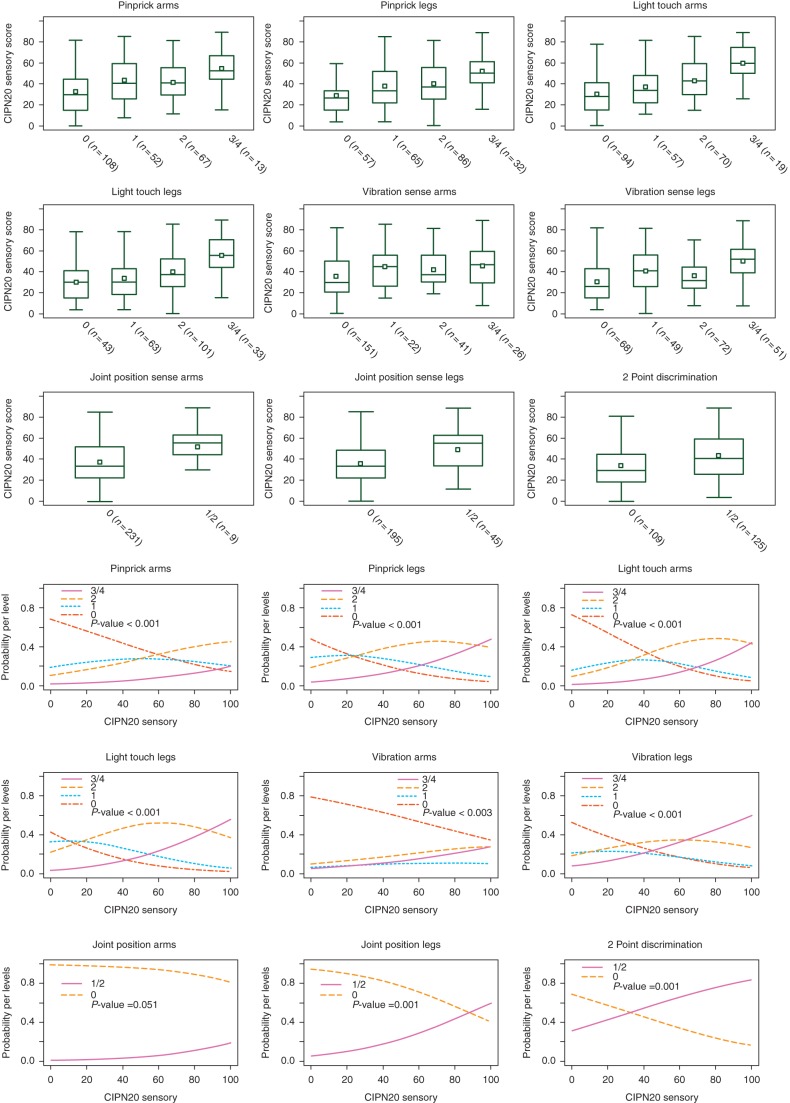
Results: Patients' probability estimates showed that the EORTC QLQ-CIPN20 sensory score was overall more highly related to the NCI-CTC sensory score. However, the vibration perception item of the TNSc had a higher probability to be scored 0 for EORTC QLQ-CIPN20 scores lower than 35, as vibration score 2 for EORTC QLQ-CIPN20 scores between 35 and 50 and as grade 3 or 4 for EORTC QLQ-CIPN20 scores higher than 50. The linear models showed a significant trend between each mISS item and increasing EORTC QLQ-CIPN20 sensory scores.
Conclusion: None of the clinical items had a perfect relationship with patients' perception, and most of the discrepancies stood in the intermediate levels of CIPN severity. Our data indicate that to achieve a comprehensive knowledge of CIPN including a reliable assessment of both the severity and the quality of CIPN-related sensory impairment, clinical and PRO measures should be always combined.
Keywords: assessment; chemotherapy; neuropathy; neurotoxicity; patient-reported outcome measure.
Figures
References
-
- Frigeni B, Piatti M, Lanzani F, et al. Chemotherapy-induced peripheral neurotoxicity can be misdiagnosed by the National Cancer Institute Common Toxicity scale. J Peripher Nerv Syst. 2011;16:228–236. - PubMed
-
- Cavaletti G, Frigeni B, Lanzani F, et al. Chemotherapy-Induced Peripheral Neurotoxicity assessment: a critical revision of the currently available tools. Eur J Cancer. 2010;46:479–494. - PubMed
-
- Cavaletti G, Frigeni B, Lanzani F, et al. The Total Neuropathy Score as an assessment tool for grading the course of chemotherapy-induced peripheral neurotoxicity: comparison with the National Cancer Institute-Common Toxicity Scale. J Peripher Nerv Syst. 2007;12:210–215. - PubMed
-
- Cavaletti G, Bogliun G, Marzorati L, et al. Grading of chemotherapy-induced peripheral neurotoxicity using the Total Neuropathy Scale. Neurology. 2003;61:1297–1300. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
