

Prognosis of patients with melanoma and microsatellitosis undergoing sentinel lymph node biopsy
- PMID: 24258854
- PMCID: PMC4001246
- DOI: 10.1245/s10434-013-3388-5
Prognosis of patients with melanoma and microsatellitosis undergoing sentinel lymph node biopsy
Abstract
Introduction: Melanoma microsatellitosis is classified as stage IIIB/C disease and is associated with a poor prognosis. Prognostic factors within this group, however, have not been well characterized.
Methods: We performed a retrospective analysis of 1,621 patients undergoing sentinel lymph node (SLN) biopsy at our institution (1996-2011) to compare patients with (n = 98) and patients without (n = 1,523) microsatellites. Univariate and multivariate logistic and Cox regression analyses were used to identify factors associated with SLN positivity and melanoma-specific survival (MSS) in patients with microsatellites.
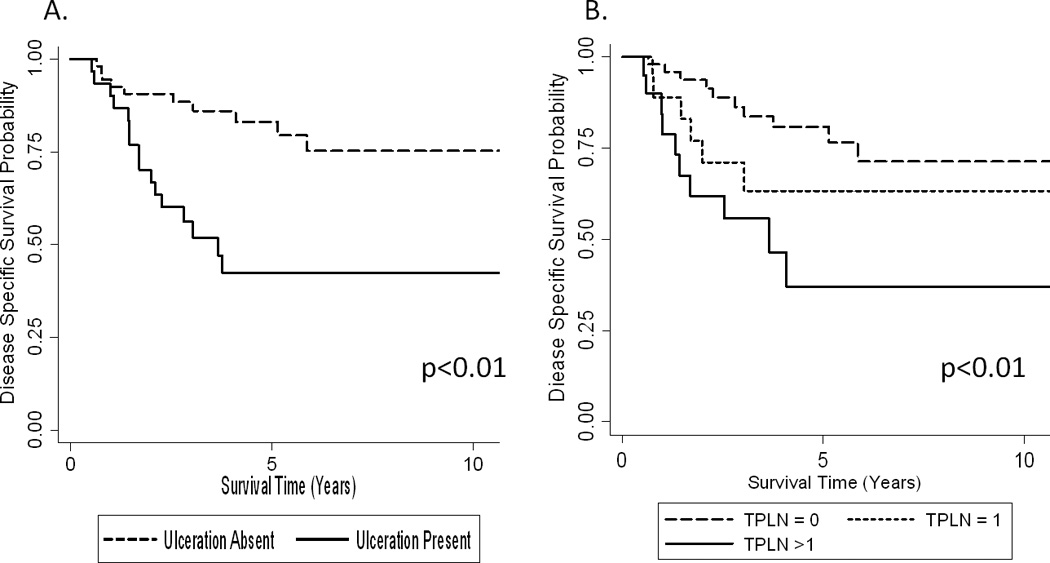
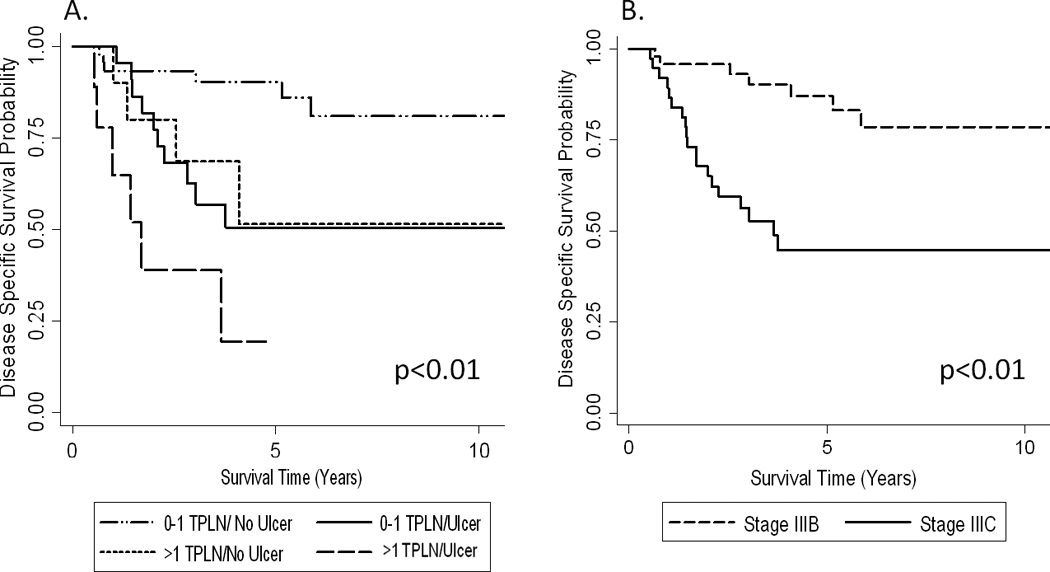
Results: Patients with microsatellites were older and had lesions with higher Clark level and greater thickness that more frequently had mitoses, ulceration, and lymphovascular invasion (LVI) (all p < 0.0001). In microsatellite patients, the SLN positivity rate was 43 %. Lesional ulceration (odds ratio [OR] = 2.9, 95 % confidence interval [CI] 1.5-8.6), absent tumor infiltrating lymphocytes (OR = 2.8, 95 % CI 1.1-7.1), and LVI (OR = 3.3, 95 % CI 1.7-10) were significantly associated with SLN positivity by multivariate analysis. With a median follow-up of 4.5 years in survivors, ulceration (hazards ratio [HR] = 3.4, 95 % CI 1.5-7.8) and >1 metastatic LN (HR = 2.7, 95 % CI 1.1-6.6) were significantly associated with decreased MSS by multivariate analysis. In patients without these prognostic factors, the 5-year MSS was 90 % (n = 49) compared with 50 % (n = 23) among patients with ulceration only, 51 % (n = 12) in those with >1 metastatic LN only, or 25 % in those with both (n = 14, p < 0.01).
Discussion: Microsatellitosis was frequently associated with multiple adverse pathologic features. In the absence of ulceration and >1 metastatic LN; however, the outcome for patients with microsatellites compared favorably to stage IIIB patients overall.
Figures
References
-
- Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med. 2006;355(13):1307–1317. - PubMed
-
- Hayes AJ, Clark MA, Harries M, Thomas JM. Management of in-transit metastases from cutaneous malignant melanoma. Br J Surg. 2004;91(6):673–682. - PubMed
-
- Murali R, Moncrieff MD, Hong J, et al. The prognostic value of tumor mitotic rate and other clinicopathologic factors in patients with locoregional recurrences of melanoma. Ann Surg Oncol. 2010;17(11):2992–2999. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
