

Pathophysiology of chronic pancreatitis
- PMID: 24259953
- PMCID: PMC3831204
- DOI: 10.3748/wjg.v19.i42.7231
Pathophysiology of chronic pancreatitis
Abstract
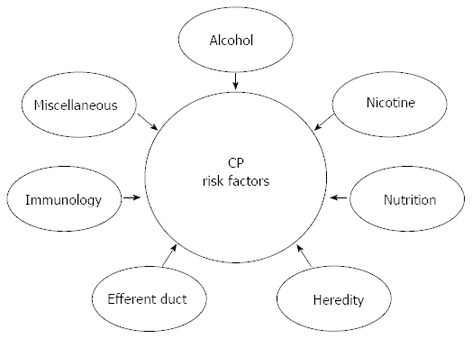
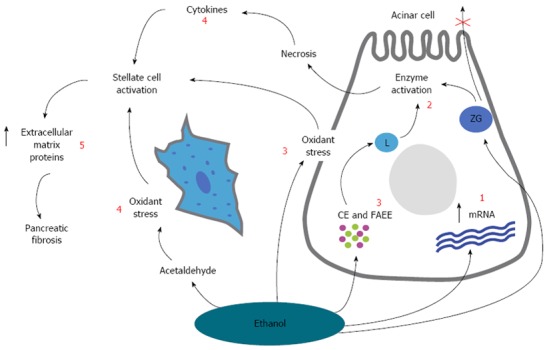
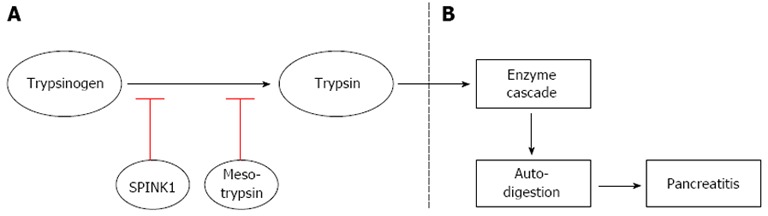
Chronic pancreatitis (CP) is an inflammatory disease of the pancreas characterized by progressive fibrotic destruction of the pancreatic secretory parenchyma. Despite the heterogeneity in pathogenesis and involved risk factors, processes such as necrosis/apoptosis, inflammation or duct obstruction are involved. This fibrosing process ultimately leads to progressive loss of the lobular morphology and structure of the pancreas, deformation of the large ducts and severe changes in the arrangement and composition of the islets. These conditions lead to irreversible morphological and structural changes resulting in impairment of both exocrine and endocrine functions. The prevalence of the disease is largely dependent on culture and geography. The etiological risk-factors associated with CP are multiple and involve both genetic and environmental factors. Throughout this review the M-ANNHEIM classification system will be used, comprising a detailed description of risk factors such as: alcohol-consumption, nicotine-consumption, nutritional factors, hereditary factors, efferent duct factors, immunological factors and miscellaneous and rare metabolic factors. Increased knowledge of the different etiological factors may encourage the use of further advanced diagnostic tools, which potentially will help clinicians to diagnose CP at an earlier stage. However, in view of the multi factorial disease and the complex clinical picture, it is not surprising that treatment of patients with CP is challenging and often unsuccessful.
Keywords: Chronic pancreatitis; Etiology; Pathogenesis; Risk factors.
Figures
References
-
- Lévy P, Barthet M, Mollard BR, Amouretti M, Marion-Audibert AM, Dyard F. Estimation of the prevalence and incidence of chronic pancreatitis and its complications. Gastroenterol Clin Biol. 2006;30:838–844. - PubMed
-
- Andersen BN, Pedersen NT, Scheel J, Worning H. Incidence of alcoholic chronic pancreatitis in Copenhagen. Scand J Gastroenterol. 1982;17:247–252. - PubMed
-
- Schneider A, Löhr JM, Singer MV. The M-ANNHEIM classification of chronic pancreatitis: introduction of a unifying classification system based on a review of previous classifications of the disease. J Gastroenterol. 2007;42:101–119. - PubMed
-
- Klöppel G, Detlefsen S, Feyerabend B. Fibrosis of the pancreas: the initial tissue damage and the resulting pattern. Virchows Arch. 2004;445:1–8. - PubMed
-
- Etemad B, Whitcomb DC. Chronic pancreatitis: diagnosis, classification, and new genetic developments. Gastroenterology. 2001;120:682–707. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
