

Ultrasonography in diagnosing chronic pancreatitis: new aspects
- PMID: 24259955
- PMCID: PMC3831206
- DOI: 10.3748/wjg.v19.i42.7247
Ultrasonography in diagnosing chronic pancreatitis: new aspects
Abstract
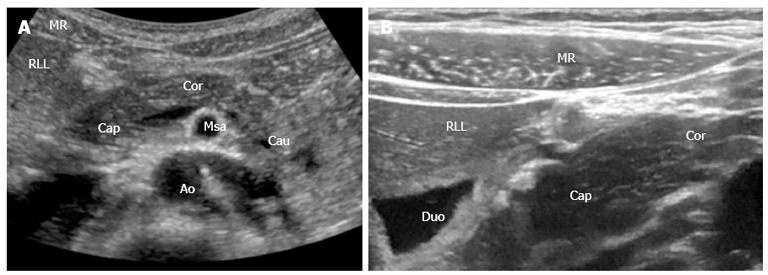
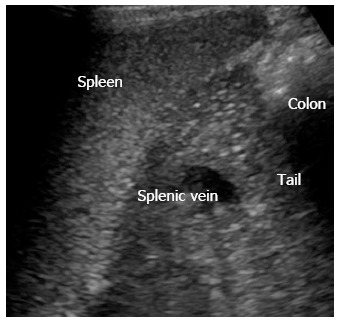
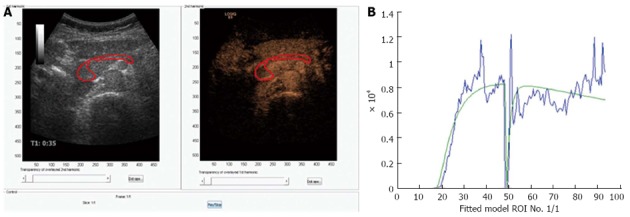
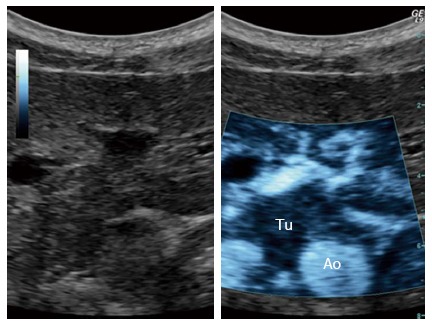
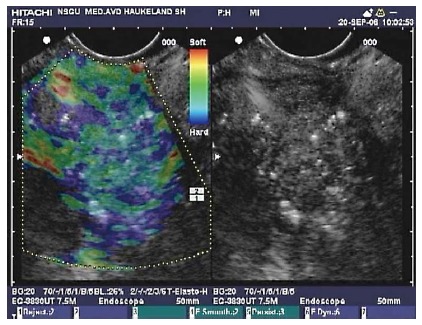
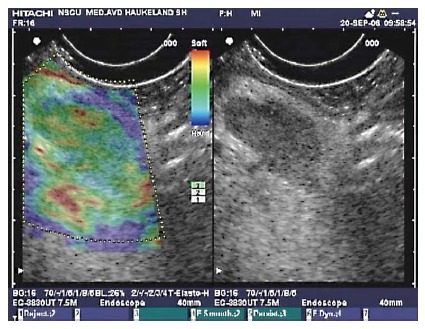
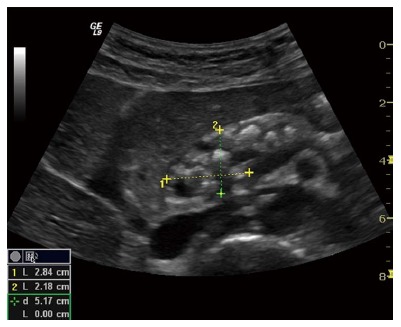
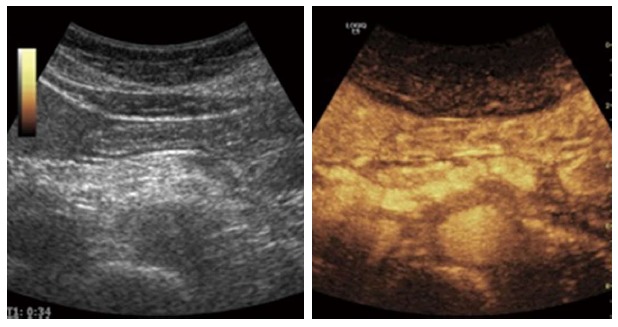
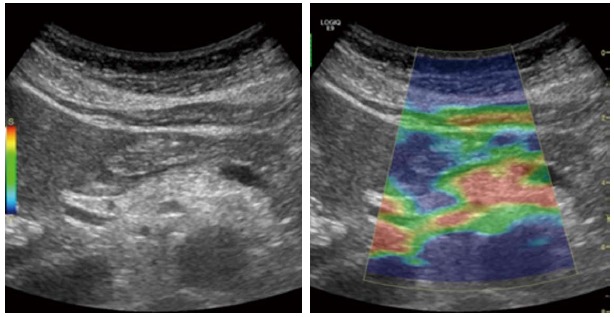
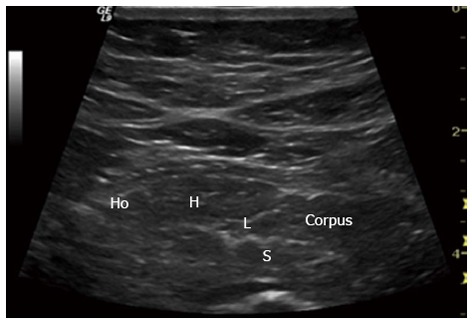
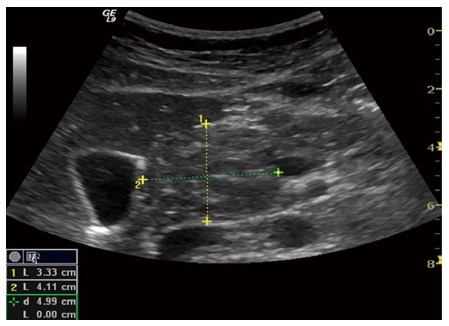
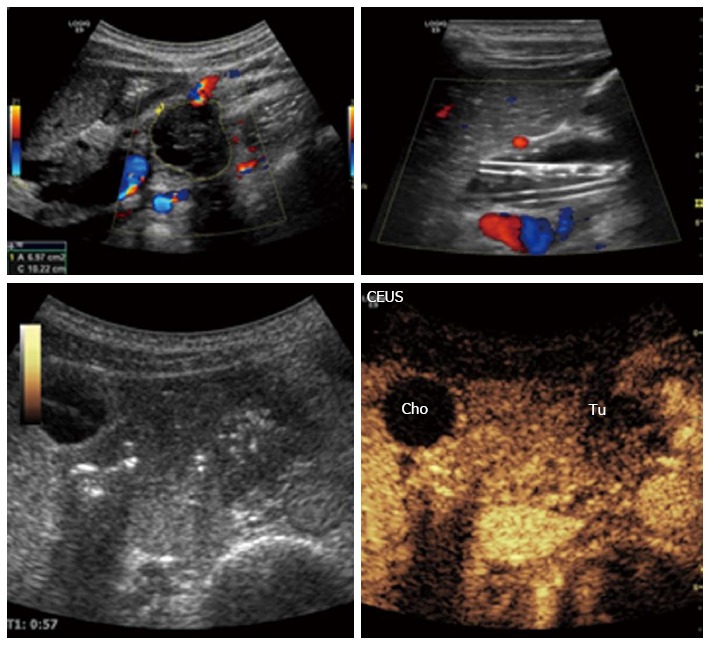
The course and outcome is poor for most patients with pancreatic diseases. Advances in pancreatic imaging are important in the detection of pancreatic diseases at early stages. Ultrasonography as a diagnostic tool has made, virtually speaking a technical revolution in medical imaging in the new millennium. It has not only become the preferred method for first line imaging, but also, increasingly to clarify the interpretation of other imaging modalities to obtain efficient clinical decision. We review ultrasonography modalities, focusing on advanced pancreatic imaging and its potential to substantially improve diagnosis of pancreatic diseases at earlier stages. In the first section, we describe scanning techniques and examination protocols. Their consequences for image quality and the ability to obtain complete and detailed visualization of the pancreas are discussed. In the second section we outline ultrasonographic characteristics of pancreatic diseases with emphasis on chronic pancreatitis. Finally, new developments in ultrasonography of the pancreas such as contrast enhanced ultrasound and elastography are enlightened.
Keywords: Chronic pancreatitis; Contrast enhanced ultrasonography; Elastography; Medical imaging technique; Pancreas; Strain imaging; Transabdominal ultrasound; Ultrasonography.
Figures
References
-
- Rösch T, Schusdziarra V, Born P, Bautz W, Baumgartner M, Ulm K, Lorenz R, Allescher HD, Gerhardt P, Siewert JR, et al. Modern imaging methods versus clinical assessment in the evaluation of hospital in-patients with suspected pancreatic disease. Am J Gastroenterol. 2000;95:2261–2270. - PubMed
-
- Swobodnik W, Meyer W, Brecht-Kraus D, Wechsler JG, Geiger S, Malfertheiner P, Junge U, Ditschuneit H. Ultrasound, computed tomography and endoscopic retrograde cholangiopancreatography in the morphologic diagnosis of pancreatic disease. Klin Wochenschr. 1983;61:291–296. - PubMed
-
- Rettenmaier G. [Methods and results of ultrasonography in the diagnosis of pancreatic diseases] Leber Magen Darm. 1972;2:88–90. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
