

Association between U.S. state AIDS Drug Assistance Program (ADAP) features and HIV antiretroviral therapy initiation, 2001-2009
- PMID: 24260137
- PMCID: PMC3832515
- DOI: 10.1371/journal.pone.0078952
Association between U.S. state AIDS Drug Assistance Program (ADAP) features and HIV antiretroviral therapy initiation, 2001-2009
Abstract
Background: U.S. state AIDS Drug Assistance Programs (ADAPs) are federally funded to provide antiretroviral therapy (ART) as the payer of last resort to eligible persons with HIV infection. States differ regarding their financial contributions to and ways of implementing these programs, and it remains unclear how this interstate variability affects HIV treatment outcomes.
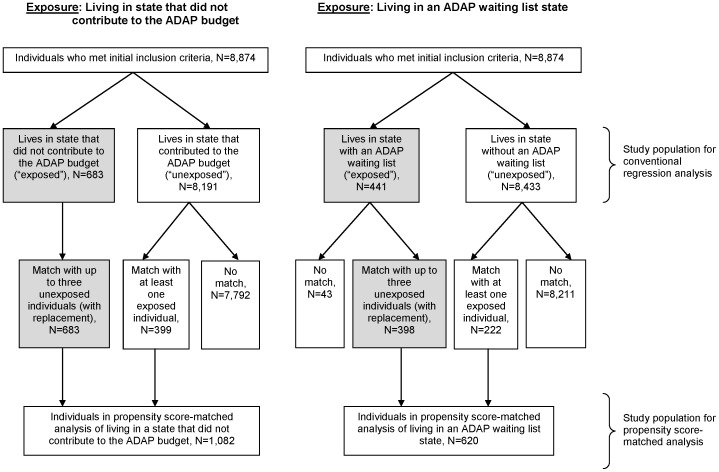
Methods: We analyzed data from HIV-infected individuals who were clinically-eligible for ART between 2001 and 2009 (i.e., a first reported CD4+ <350 cells/uL or AIDS-defining illness) from 14 U.S. cohorts of the North American AIDS Cohort Collaboration on Research and Design (NA-ACCORD). Using propensity score matching and Cox regression, we assessed ART initiation (within 6 months following eligibility) and virologic suppression (within 1 year) based on differences in two state ADAP features: the amount of state funding in annual ADAP budgets and the implementation of waiting lists. We performed an a priori subgroup analysis in persons with a history of injection drug use (IDU).
Results: Among 8,874 persons, 56% initiated ART within six months following eligibility. Persons living in states with no additional state contribution to the ADAP budget initiated ART on a less timely basis (hazard ratio [HR] 0.73, 95% CI 0.60-0.88). Living in a state with an ADAP waiting list was not associated with less timely initiation (HR 1.12, 95% CI 0.87-1.45). Neither additional state contributions nor waiting lists were significantly associated with virologic suppression. Persons with an IDU history initiated ART on a less timely basis (HR 0.67, 95% CI 0.47-0.95).
Conclusions: We found that living in states that did not contribute additionally to the ADAP budget was associated with delayed ART initiation when treatment was clinically indicated. Given the changing healthcare environment, continued assessment of the role of ADAPs and their features that facilitate prompt treatment is needed.
Conflict of interest statement
Figures

References
-
- Office of National AIDS Policy. National HIV/AIDS Strategy for the United States. Available: http://www.whitehouse.gov/administration/eop/onap/nhas. Accessed 15 Jul 2010.
-
- Centers for Disease Control and Prevention (2011) Vital signs: HIV prevention through care and treatment–United States. MMWR Morb Mortal Wkly Rep 60 (47) 1618–23. - PubMed
-
- Palella FJ, Baker RK, Buchacz K, Chmiel JS, Tedaldi EM, et al. (2011) Increased mortality among publicly insured participants in the HIV Outpatient Study despite HAART treatment. AIDS 25 (15) 1865–76. - PubMed
-
- Shapiro MF, Morton SC, McCaffrey DF, Senterfitt JW, Fleishman JA, et al. (1999) Variations in the care of HIV-infected adults in the United States: Results from the HIV Cost and Services Utilization Study. JAMA 281 (24) 2305–15. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01-AI35043/AI/NIAID NIH HHS/United States
- K24 DA000432/DA/NIDA NIH HHS/United States
- K24-DA00432/DA/NIDA NIH HHS/United States
- P30-AI27757/AI/NIAID NIH HHS/United States
- P30 AI036219/AI/NIAID NIH HHS/United States
- R01 AA016893/AA/NIAAA NIH HHS/United States
- U01-AI34989/AI/NIAID NIH HHS/United States
- P30 AI027767/AI/NIAID NIH HHS/United States
- U01 AI035042/AI/NIAID NIH HHS/United States
- U01 DA036297/DA/NIDA NIH HHS/United States
- F31 DA030254/DA/NIDA NIH HHS/United States
- CBR-86906/CAPMC/ CIHR/Canada
- R01-AA16893/AA/NIAAA NIH HHS/United States
- M01 RR000079/RR/NCRR NIH HHS/United States
- R24-AI067039/AI/NIAID NIH HHS/United States
- U01 AI037984/AI/NIAID NIH HHS/United States
- U01-HD32632/HD/NICHD NIH HHS/United States
- R01 DA011602/DA/NIDA NIH HHS/United States
- K01 AI071725/AI/NIAID NIH HHS/United States
- P30-AI27763/AI/NIAID NIH HHS/United States
- U01-AI34993/AI/NIAID NIH HHS/United States
- M01-RR00083/RR/NCRR NIH HHS/United States
- TGF-96118/CAPMC/ CIHR/Canada
- U01 AI031834/AI/NIAID NIH HHS/United States
- HCP-97105/CAPMC/ CIHR/Canada
- K01-AI071754/AI/NIAID NIH HHS/United States
- M01-RR00079/RR/NCRR NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- G12 MD007583/MD/NIMHD NIH HHS/United States
- P30 AI054999/AI/NIAID NIH HHS/United States
- R01-DA04334/DA/NIDA NIH HHS/United States
- U01-AI35040/AI/NIAID NIH HHS/United States
- R01 DA004334/DA/NIDA NIH HHS/United States
- U01-AI37984/AI/NIAID NIH HHS/United States
- M01-RR00071/RR/NCRR NIH HHS/United States
- U01-AI35004/AI/NIAID NIH HHS/United States
- CDC200-2006-18797/PHS HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- P30-AI036219/AI/NIAID NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01 AI037613/AI/NIAID NIH HHS/United States
- KRS-86251/CAPMC/ CIHR/Canada
- M01 RR000071/RR/NCRR NIH HHS/United States
- AHQ290-01-0012/PHS HHS/United States
- U01-AI35042/AI/NIAID NIH HHS/United States
- M01 RR000722/RR/NCRR NIH HHS/United States
- M01-RR025747/RR/NCRR NIH HHS/United States
- CBR-94036/CAPMC/ CIHR/Canada
- U01 AI035041/AI/NIAID NIH HHS/United States
- R24 AI067039/AI/NIAID NIH HHS/United States
- U01-AI37613/AI/NIAID NIH HHS/United States
- M01-RR-00052/RR/NCRR NIH HHS/United States
- U01-AI069918/AI/NIAID NIH HHS/United States
- K24-AI1065298/AI/NIAID NIH HHS/United States
- U01-AI42590/AI/NIAID NIH HHS/United States
- K01 AI071754/AI/NIAID NIH HHS/United States
- P30-AI50410/AI/NIAID NIH HHS/United States
- UL1-RR024131/RR/NCRR NIH HHS/United States
- R01-DA12568/DA/NIDA NIH HHS/United States
- U01-AI31834/AI/NIAID NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- K01 AI093197/AI/NIAID NIH HHS/United States
- U01 AI069918/AI/NIAID NIH HHS/United States
- U01-AI35041/AI/NIAID NIH HHS/United States
- N02 CP055504/CP/NCI NIH HHS/United States
- U01 AI035043/AI/NIAID NIH HHS/United States
- K23-AI610320/AI/NIAID NIH HHS/United States
- P30 AI027757/AI/NIAID NIH HHS/United States
- UL1 RR025747/RR/NCRR NIH HHS/United States
- U01-AI35039/AI/NIAID NIH HHS/United States
- R01 DA012568/DA/NIDA NIH HHS/United States
- N02-CP55504/CP/NCI NIH HHS/United States
- F31-DA30254/DA/NIDA NIH HHS/United States
- P30-AI27767/AI/NIAID NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- K01-AI093197/AI/NIAID NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- R01-DA11602/DA/NIDA NIH HHS/United States
- M01 RR000083/RR/NCRR NIH HHS/United States
- K01-AI071725/AI/NIAID NIH HHS/United States
- U01-AI34994/AI/NIAID NIH HHS/United States
- 169621/CAPMC/ CIHR/Canada
- U01 AI035039/AI/NIAID NIH HHS/United States
- M01-RR00722/RR/NCRR NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
- P30-AI54999/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
