

Macular cone abnormalities in retinitis pigmentosa with preserved central vision using adaptive optics scanning laser ophthalmoscopy
- PMID: 24260224
- PMCID: PMC3834127
- DOI: 10.1371/journal.pone.0079447
Macular cone abnormalities in retinitis pigmentosa with preserved central vision using adaptive optics scanning laser ophthalmoscopy
Abstract
Purpose: To assess macular photoreceptor abnormalities in eyes with retinitis pigmentosa (RP) with preserved central vision using adaptive optics scanning laser ophthalmoscopy (AO-SLO).
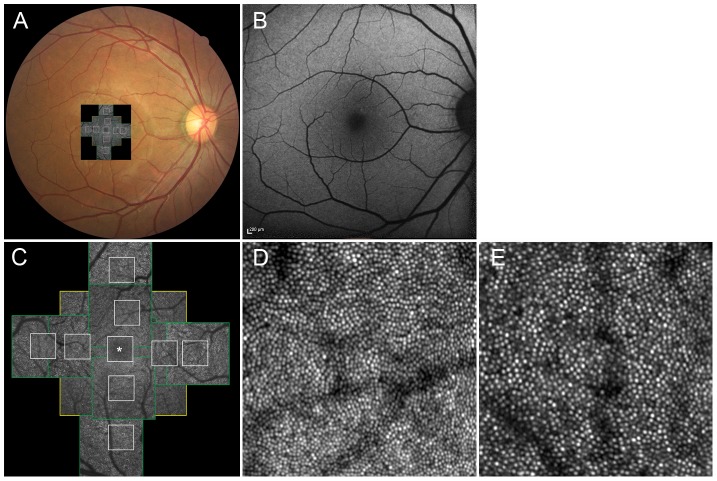
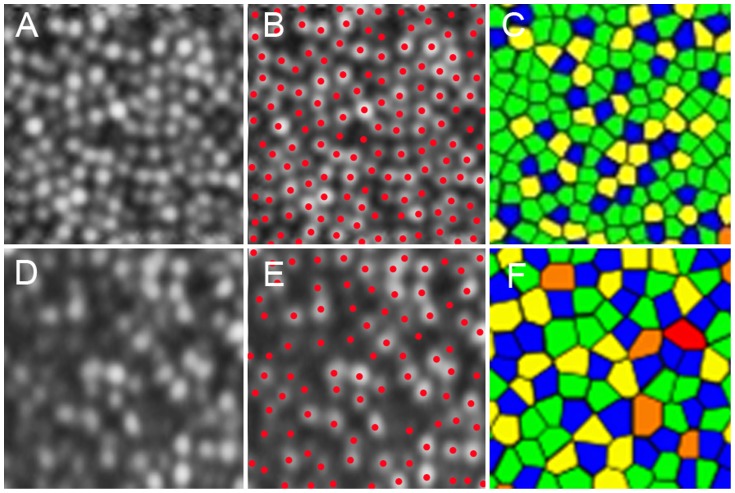
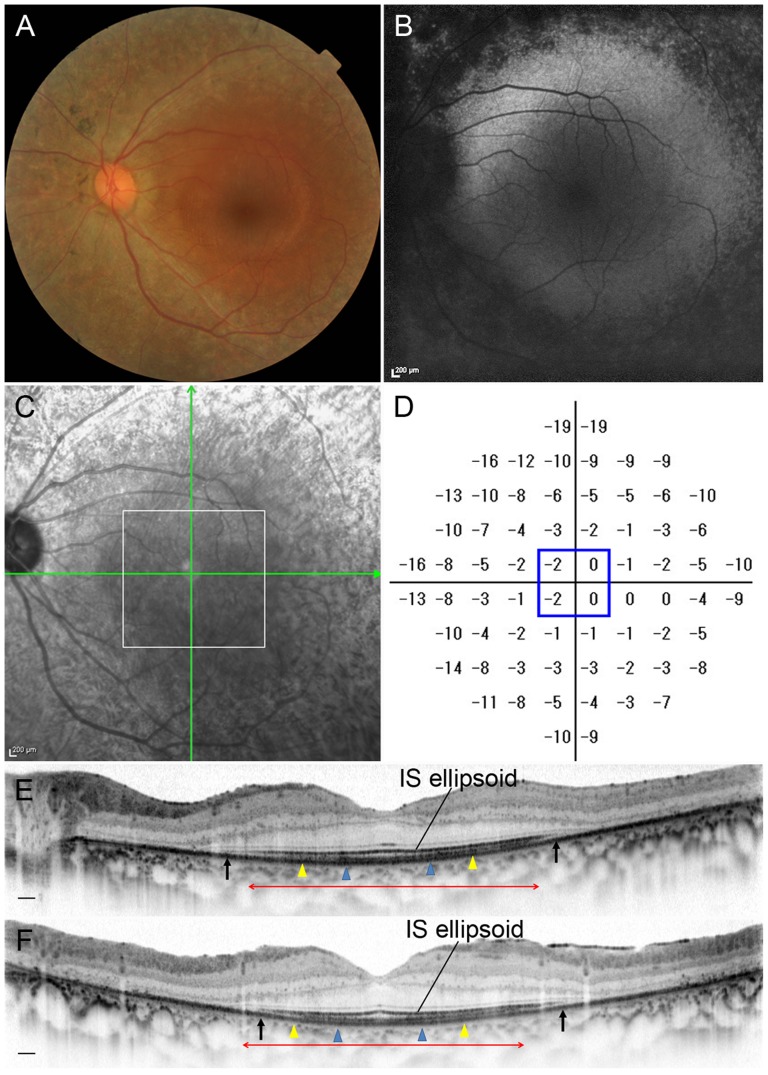
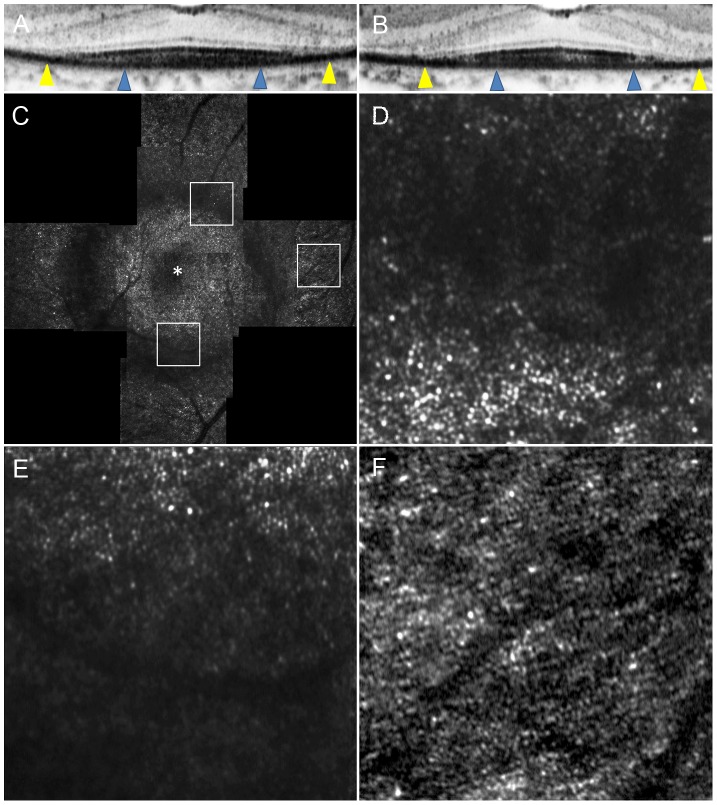
Methods: Fourteen eyes of 14 patients with RP (best-corrected visual acuity 20/20 or better) and 12 eyes of 12 volunteers underwent a full ophthalmologic examination, fundus autofluorescence, spectral-domain optical coherence tomography (SD-OCT), and imaging with a prototype AO-SLO system. Cone density and spatial organization of the cone mosaic were assessed using AO-SLO images.
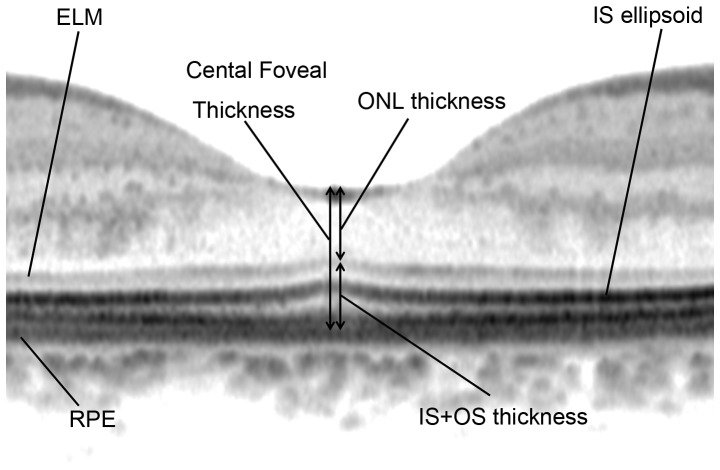
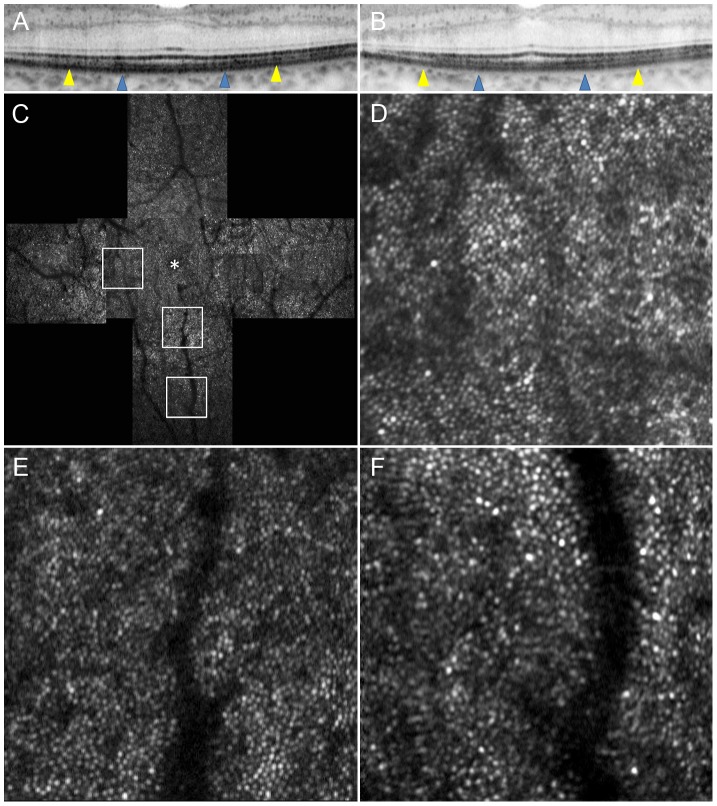
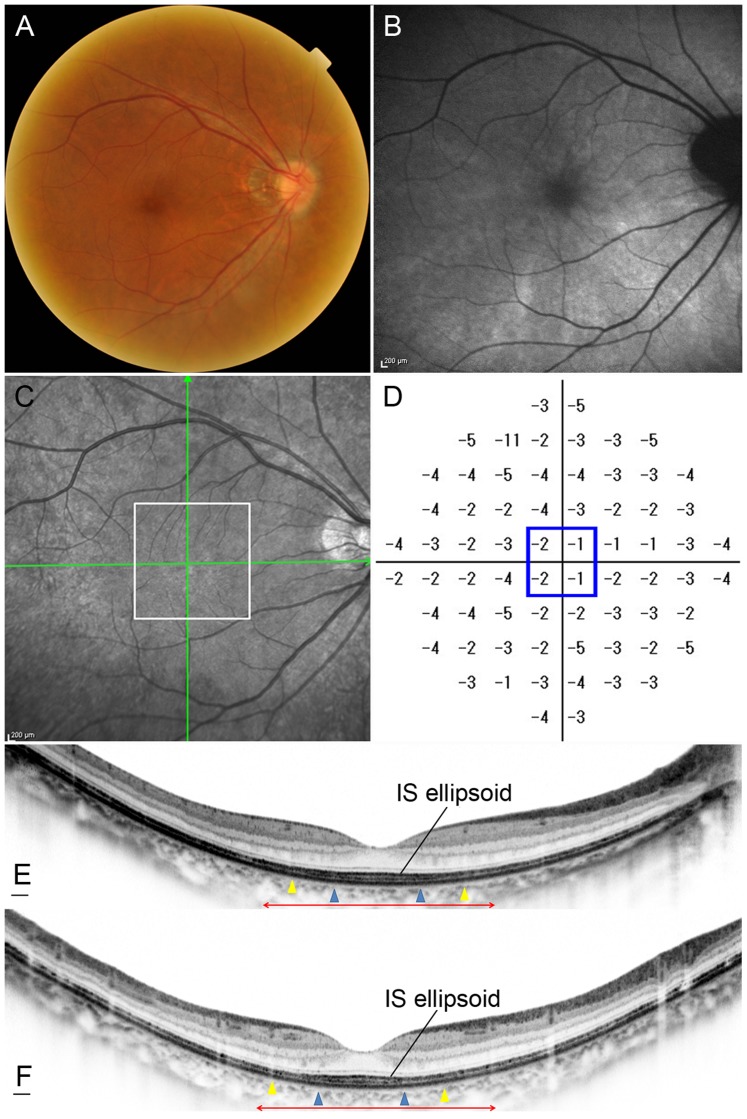
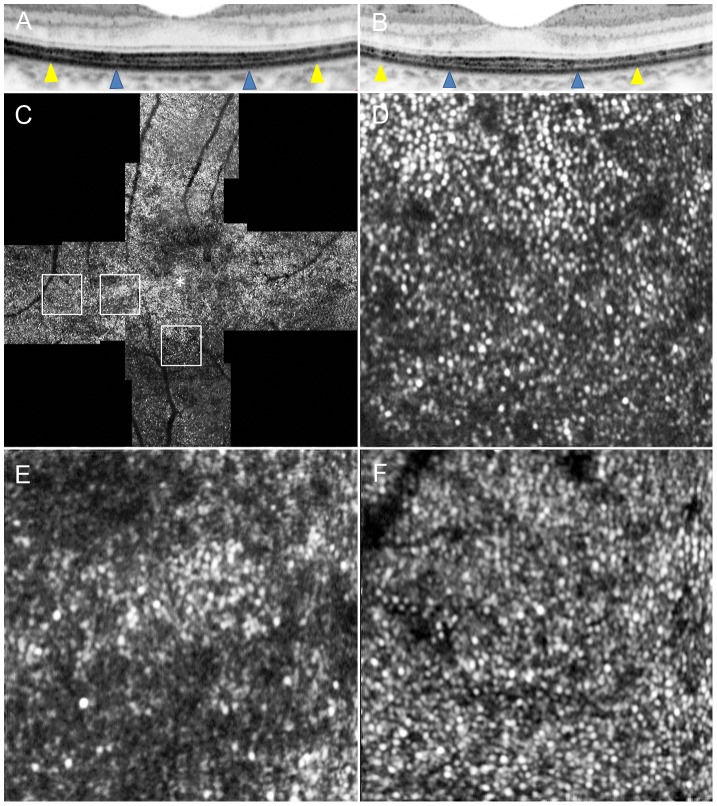
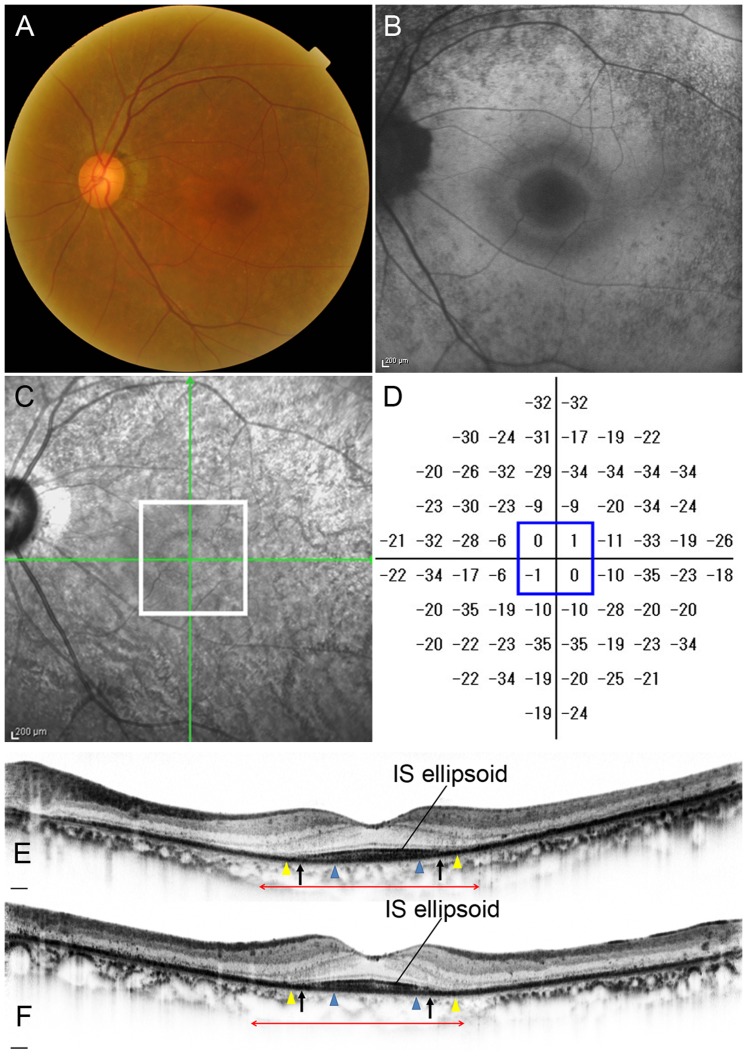
Results: In 3 eyes with RP and preserved central vision, cones formed a mostly regular mosaic pattern with small patchy dark areas, and in 10 eyes, the cone mosaic patterns were less regular, and large dark regions with missing cones were apparent. Only one eye with RP demonstrated a normal, regular cone mosaic pattern. In eyes with RP, cone density was significantly lower at 0.5 mm and 1.0 mm from the center of the fovea compared to normal eyes (P<0.001 and 0.021, respectively). At 0.5 mm and 1.0 mm from the center of the fovea, a decreased number of cones had 6 neighbors in eyes with RP (P = 0.002 for both). Greater decrease in cone density was related to disruption of the photoreceptor inner segment (IS) ellipsoid band on SD-OCT images (P = 0.044); however, dark regions were seen on AO-SLO even in areas of continuous IS ellipsoid on SD-OCT. Decreased cone density correlated thinner outer nuclear layer (P = 0.029) and thinner inner segment and outer segment thickness (P = 0.011) on SD-OCT.
Conclusions: Cone density is decreased and the regularity of the cone mosaic spatial arrangement is disrupted in eyes with RP, even when visual acuity and foveal sensitivity are good. AO-SLO imaging is a sensitive quantitative tool for detecting photoreceptor abnormalities in eyes with RP.
Conflict of interest statement
Figures
References
-
- Berson EL (1993) Retinitis pigmentosa. The Friedenwald Lecture. Invest Ophthalmol Vis Sci 34: 1659–1676. - PubMed
-
- Hartong DT, Berson EL, Dryja TP (2006) Retinitis pigmentosa. Lancet 368: 1795–1809. - PubMed
-
- Grover S, Fishman GA, Anderson RJ, Alexander KR, Derlacki DJ (1997) Rate of visual field loss in retinitis pigmentosa. Ophthalmology 104: 460–465. - PubMed
-
- Hamada S, Yoshida K, Chihara E (2000) Optical coherence tomography images of retinitis pigmentosa. Ophthalmic Surg Lasers 31: 253–256. - PubMed
-
- Rumen F, Souied E, Oubraham H, Coscas G, Soubrane G (2001) [Optical coherence tomography in the follow up of macular edema treatment in retinitis pigmentosa]. J Fr Ophtalmol 24: 854–859. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
