

Concepts of scientific integrative medicine applied to the physiology and pathophysiology of catecholamine systems
- PMID: 24265239
- PMCID: PMC4902023
- DOI: 10.1002/cphy.c130006
Concepts of scientific integrative medicine applied to the physiology and pathophysiology of catecholamine systems
Abstract
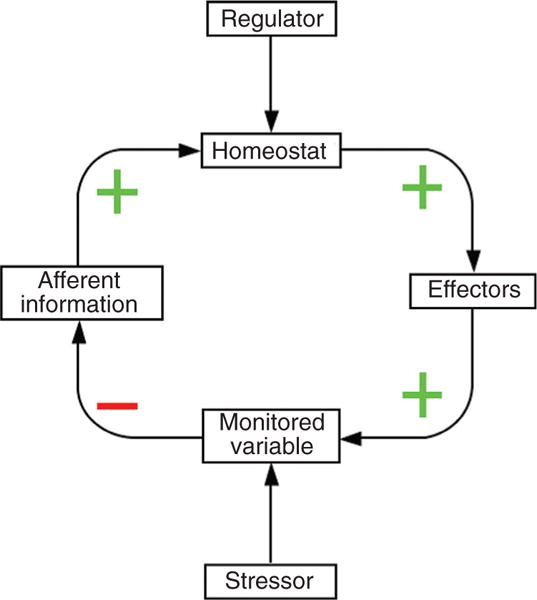
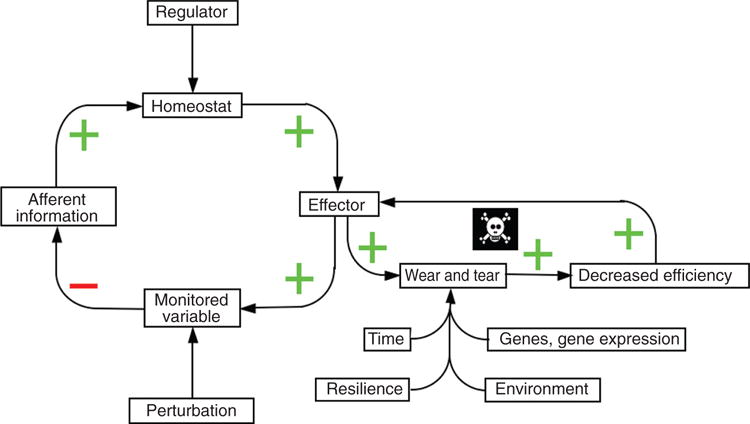
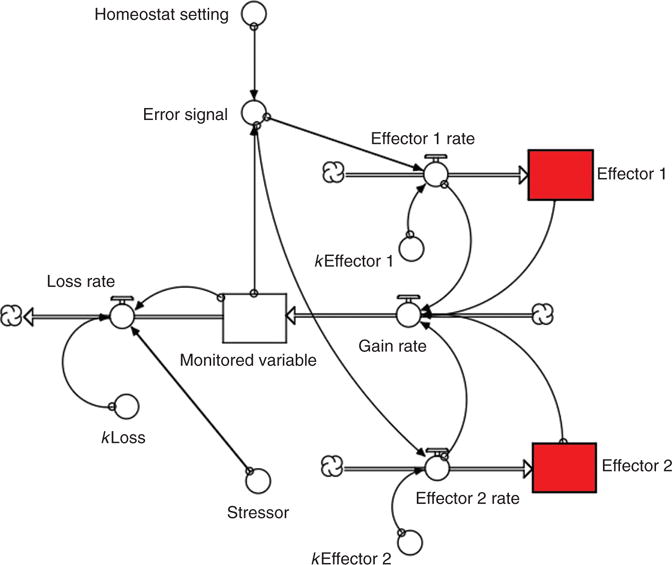
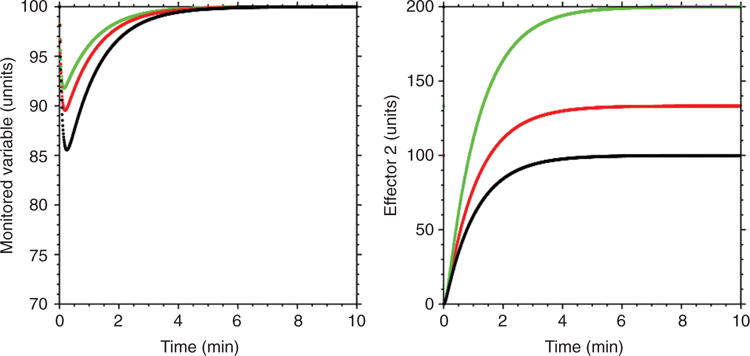
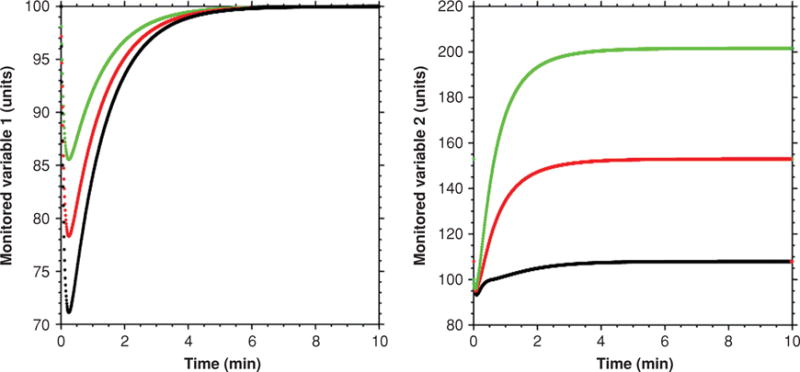
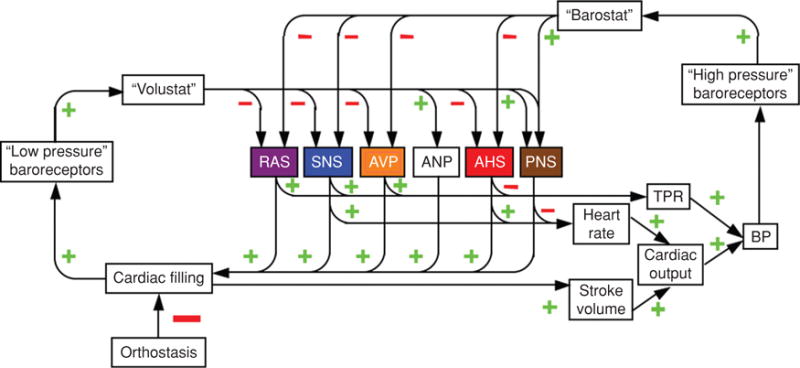
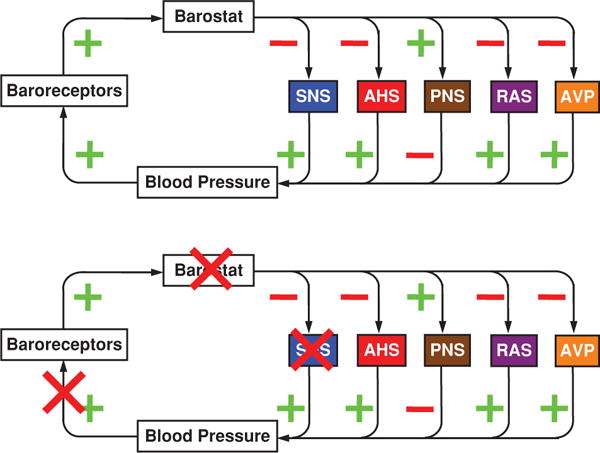
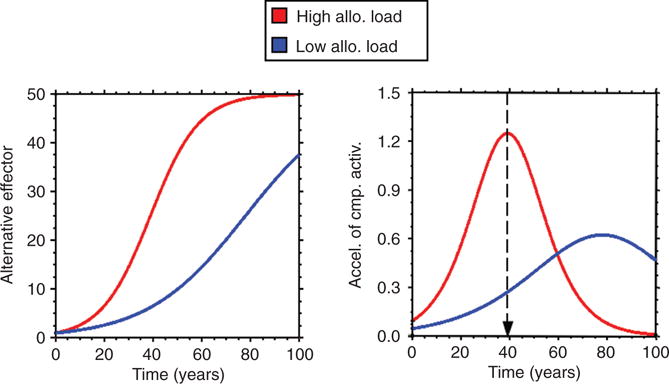
This review presents concepts of scientific integrative medicine and relates them to the physiology of catecholamine systems and to the pathophysiology of catecholamine-related disorders. The applications to catecholamine systems exemplify how scientific integrative medicine links systems biology with integrative physiology. Concepts of scientific integrative medicine include (i) negative feedback regulation, maintaining stability of the body's monitored variables; (ii) homeostats, which compare information about monitored variables with algorithms for responding; (iii) multiple effectors, enabling compensatory activation of alternative effectors and primitive specificity of stress response patterns; (iv) effector sharing, accounting for interactions among homeostats and phenomena such as hyperglycemia attending gastrointestinal bleeding and hyponatremia attending congestive heart failure; (v) stress, applying a definition as a state rather than as an environmental stimulus or stereotyped response; (vi) distress, using a noncircular definition that does not presume pathology; (vii) allostasis, corresponding to adaptive plasticity of feedback-regulated systems; and (viii) allostatic load, explaining chronic degenerative diseases in terms of effects of cumulative wear and tear. From computer models one can predict mathematically the effects of stress and allostatic load on the transition from wellness to symptomatic disease. The review describes acute and chronic clinical disorders involving catecholamine systems-especially Parkinson disease-and how these concepts relate to pathophysiology, early detection, and treatment and prevention strategies in the post-genome era.
Published 2013. Compr Physiol 3:1569-1610, 2013.
Figures


























Similar articles
-
Neurocardiology: therapeutic implications for cardiovascular disease.Cardiovasc Ther. 2012 Apr;30(2):e89-106. doi: 10.1111/j.1755-5922.2010.00244.x. Epub 2010 Nov 25. Cardiovasc Ther. 2012. PMID: 21108771 Free PMC article. Review.
-
Stress, allostatic load, catecholamines, and other neurotransmitters in neurodegenerative diseases.Cell Mol Neurobiol. 2012 Jul;32(5):661-6. doi: 10.1007/s10571-011-9780-4. Cell Mol Neurobiol. 2012. PMID: 22297542 Free PMC article. Review.
-
Computer models of stress, allostasis, and acute and chronic diseases.Ann N Y Acad Sci. 2008 Dec;1148:223-31. doi: 10.1196/annals.1410.061. Ann N Y Acad Sci. 2008. PMID: 19120114 Free PMC article.
-
Stress, allostatic load, catecholamines, and other neurotransmitters in neurodegenerative diseases.Endocr Regul. 2011 Apr;45(2):91-8. doi: 10.4149/endo_2011_02_91. Endocr Regul. 2011. PMID: 21615193 Free PMC article. Review.
-
How does homeostasis happen? Integrative physiological, systems biological, and evolutionary perspectives.Am J Physiol Regul Integr Comp Physiol. 2019 Apr 1;316(4):R301-R317. doi: 10.1152/ajpregu.00396.2018. Epub 2019 Jan 16. Am J Physiol Regul Integr Comp Physiol. 2019. PMID: 30649893 Free PMC article. Review.
Cited by
-
Alpha2-adrenoceptors in adrenomedullary chromaffin cells: functional role and pathophysiological implications.Pflugers Arch. 2018 Jan;470(1):61-66. doi: 10.1007/s00424-017-2059-y. Epub 2017 Aug 23. Pflugers Arch. 2018. PMID: 28836008 Review.
-
Calculating Stress: From Entropy to a Thermodynamic Concept of Health and Disease.PLoS One. 2016 Jan 15;11(1):e0146667. doi: 10.1371/journal.pone.0146667. eCollection 2016. PLoS One. 2016. PMID: 26771542 Free PMC article.
-
Homeostatic systems, biocybernetics, and autonomic neuroscience.Auton Neurosci. 2017 Dec;208:15-28. doi: 10.1016/j.autneu.2017.09.001. Epub 2017 Sep 5. Auton Neurosci. 2017. PMID: 28918243 Free PMC article. Review.
-
Biochemical and Functional Changes in the Eye As a Manifestation of Systemic Degeneration of the Nervous System in Parkinsonism.Acta Naturae. 2018 Jul-Sep;10(3):62-67. Acta Naturae. 2018. PMID: 30397528 Free PMC article.
-
Autonomic Cardiovascular Control in Health and Disease.Compr Physiol. 2023 Mar 30;13(2):4493-4511. doi: 10.1002/cphy.c210037. Compr Physiol. 2023. PMID: 36994768 Free PMC article. Review.
References
-
- Abboud FM. Neurocardiogenic syncope. N Engl J Med. 1993;328:1117–1120. - PubMed
-
- Aicher SA, Kurucz OS, Reis DJ, Milner TA. Nucleus tractus solitarius efferent terminals synapse on neurons in the caudal ventrolateral medulla that project to the rostral ventrolateral medulla. Brain Res. 1995;693:51–63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
