

Detection of mutations in KLHL3 and CUL3 in families with FHHt (familial hyperkalaemic hypertension or Gordon's syndrome)
- PMID: 24266877
- PMCID: PMC3963521
- DOI: 10.1042/CS20130326
Detection of mutations in KLHL3 and CUL3 in families with FHHt (familial hyperkalaemic hypertension or Gordon's syndrome)
Abstract
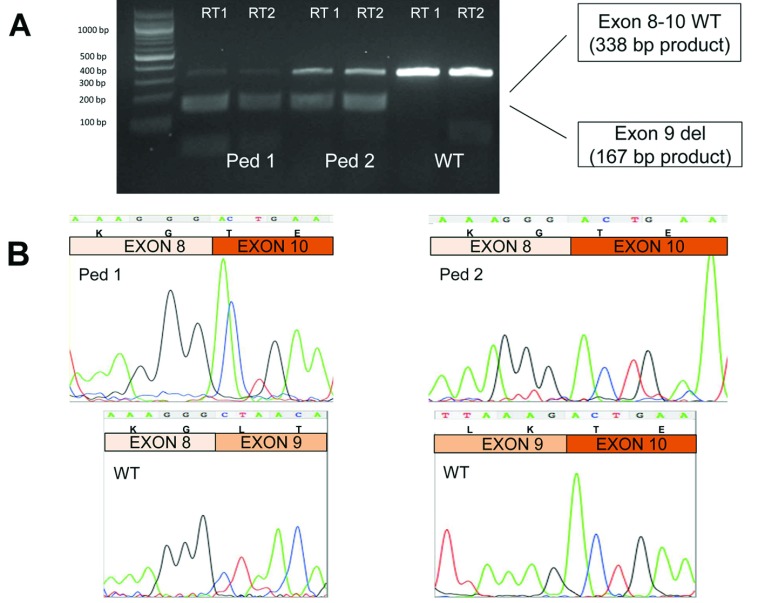
The study of families with rare inherited forms of hypo- and hyper-tension has been one of the most successful strategies to probe the molecular pathophysiology of blood pressure control and has revealed dysregulation of distal nephron Na+ reabsorption to be a common mechanism. FHHt (familial hyperkalaemic hypertension; also known as Gordon's syndrome) is a salt-dependent form of hypertension caused by mutations in the regulators of the thiazide-sensitive Na+-Cl- co-transporter NCC [also known as SLC12A3 (solute carrier family 12 member 3)] and is effectively treated by thiazide diuretics and/or dietary salt restriction. Variation in at least four genes can cause FHHt, including WNK1 [With No lysine (=K) 1] and WNK4, KLHL3 (kelch-like family member 3), and CUL3 (cullin 3). In the present study we have identified novel disease-causing variants in CUL3 and KLHL3 segregating in 63% of the pedigrees with previously unexplained FHHt, confirming the importance of these recently described FHHt genes. We have demonstrated conclusively, in two unrelated affected individuals, that rare intronic variants in CUL3 cause the skipping of exon 9 as has been proposed previously. KLHL3 variants all occur in kelch-repeat domains and so probably disrupt WNK complex binding. We have found no evidence of any plausible disease-causing variants within SLC4A8 (an alternative thiazide-sensitive sodium transporter) in this population. The results of the present study support the existing evidence that the CUL3 and KLHL3 gene products are physiologically important regulators of thiazide-sensitive distal nephron NaCl reabsorption, and hence potentially interesting novel anti-hypertensive drug targets. As a third of our non-WNK FHHt families do not have plausible CUL3 or KLHL3 variants, there are probably additional, as yet undiscovered, regulators of the thiazide-sensitive pathways.
Figures
References
-
- World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Life. Geneva: World Health Organization; 2002. ( http:://www.who.int/whr/2002/en/) - PubMed
-
- World Health Organization. Global Status Report on Noncommunicable Diseases 2010. Geneva: World Health Oraganization; 2010. ( http:://www.who.int/nmh/publications/ncd_report_full_en.pdf)
-
- Cardiovascular Health Working Group of the Faculty of Public Health. Easing the Pressure: Tackling Hypertension. London: Faculty of Public Health and the National Heart Forum; 2005. ( http:://www.fph.org.uk/uploads/hypertendion_all.pdf)
-
- Lifton R. P., Gharavi A. G., Geller D. S. Molecular mechanisms of human hypertension. Cell. 2001;104:545–556. - PubMed
-
- Glover M., Mercier Zuber A., O’Shaughnessy K. M. Hypertension, dietary salt intake, and the role of the thiazide-sensitive sodium chloride transporter NCCT. Cardiovasc. Ther. 2011;29:68–76. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials