

Tranexamic acid for patients with traumatic brain injury: a randomized, double-blinded, placebo-controlled trial
- PMID: 24267513
- PMCID: PMC4221638
- DOI: 10.1186/1471-227X-13-20
Tranexamic acid for patients with traumatic brain injury: a randomized, double-blinded, placebo-controlled trial
Abstract
Background: Traumatic brain injury (TBI) is commonly accompanied by intracranial bleeding which can worsen after hospital admission. Tranexamic acid (TXA) has been shown to reduce bleeding in elective surgery and there is evidence that short courses of TXA can reduce rebleeding in spontaneous intracranial haemorrhage. We aimed to determine the effectiveness and safety of TXA in preventing progressive intracranial haemorrhage in TBI.
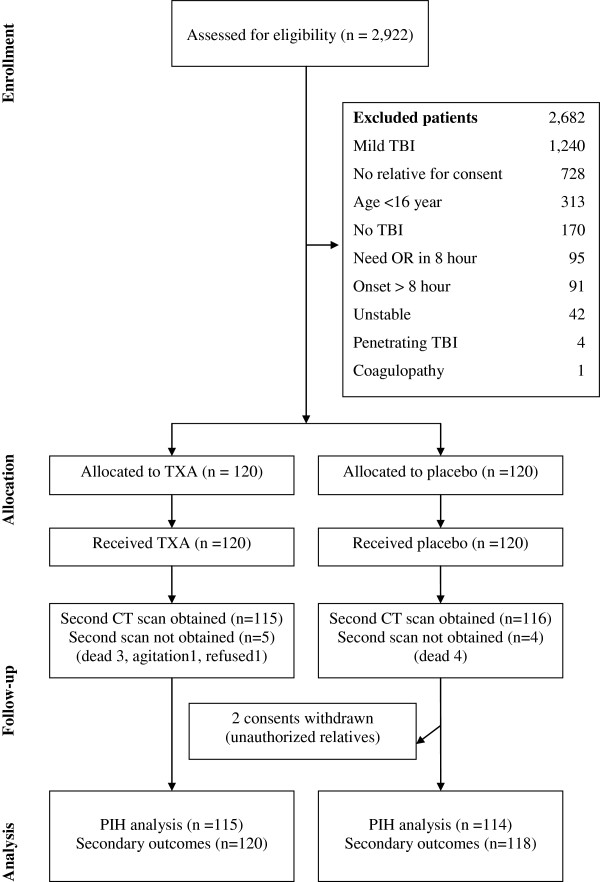
Methods: This is a double blinded, placebo controlled randomized trial. We enrolled 238 patients older than 16 years with moderate to severe TBI (post-resuscitation Glasgow Coma Scale (GCS) 4 to 12) who had a computerized tomography (CT) brain scan within eight hours of injury and in whom there was no immediate indication for surgery. We excluded patients if they had a coagulopathy or a serum creatinine over than 2.0 milligrams%. The treatment was a single dose of 2 grams of TXA in addition to other standard treatments. The primary outcome was progressive intracranial haemorrhage (PIH) which was defined as an intracranial haemorrhage seen on the second CT scan that was not seen on the first CT scan, or an intracranial haemorrhage seen on the first scan that had expanded by 25% or more on any dimension (height, length, or width) on the second scan.
Results: Progressive intracranial haemorrhage was present in 21 (18%) of 120 patients allocated to TXA and in 32 (27%) of 118 patients allocated to placebo. The difference was not statistically significant [RR = 0.65 (95% CI 0.40 to 1.05)]. There were no significant difference in the risk of death from all causes in patients allocated to TXA compared with placebo [RR = 0.69 (95% CI 0.35 to 1.39)] and the risk of unfavourable outcome on the Glasgow Outcome Scale [RR = 0.76 (95% CI 0.46 to 1.27)]. There was no evidence of increased risk of thromboembolic events in those patients allocated to TXA.
Conclusions: TXA may reduce PIH in patients with TBI; however, the difference was not statistically significant in this trial. Large clinical trials are needed to confirm and to assess the effect of TXA on death or disability after TBI.
References
-
- Bruns J Jr, Hauser WA. The epidemiology of traumatic brain injury: a review. Epilepsia. 2003;44(Suppl 10):2–10. - PubMed
-
- Yutthakasemsunt S. Study in traumatic brain injury outcome study in Khon Kaen hospital: analysis of clinical factors and outcomes [In Thai] J Trauma. 2006;25/2:53–75.
-
- Bullock MR, Chesnut R, Ghajar J, Gordon D, Hartl R, Newell DW, Servadei F, Walters BC, Wilberger JE. Introduction. Neurosurger. 2006;58(3 Suppl):S1–S3. discussion Si-iv. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
