

Outcomes of antiretroviral treatment programmes in rural Lesotho: health centres and hospitals compared
- PMID: 24267671
- PMCID: PMC3838571
- DOI: 10.7448/IAS.16.1.18616
Outcomes of antiretroviral treatment programmes in rural Lesotho: health centres and hospitals compared
Abstract
Introduction: Lesotho was among the first countries to adopt decentralization of care from hospitals to nurse-led health centres (HCs) to scale up the provision of antiretroviral therapy (ART). We compared outcomes between patients who started ART at HCs and hospitals in two rural catchment areas in Lesotho.
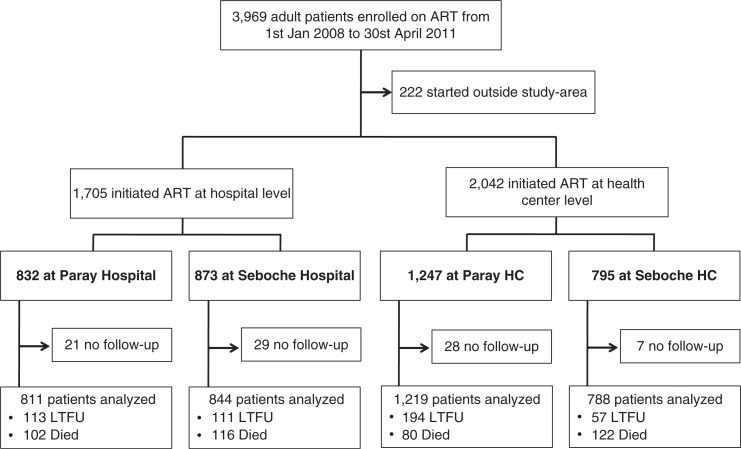
Methods: The two catchment areas comprise two hospitals and 12 HCs. Patients ≥16 years starting ART at a hospital or HC between 2008 and 2011 were included. Loss to follow-up (LTFU) was defined as not returning to the facility for ≥180 days after the last visit, no follow-up (no FUP) as not returning after starting ART, and retention in care as alive and on ART at the facility. The data were analysed using logistic regression, competing risk regression and Kaplan-Meier methods. Multivariable analyses were adjusted for sex, age, CD4 cell count, World Health Organization stage, catchment area and type of ART. All analyses were stratified by gender.
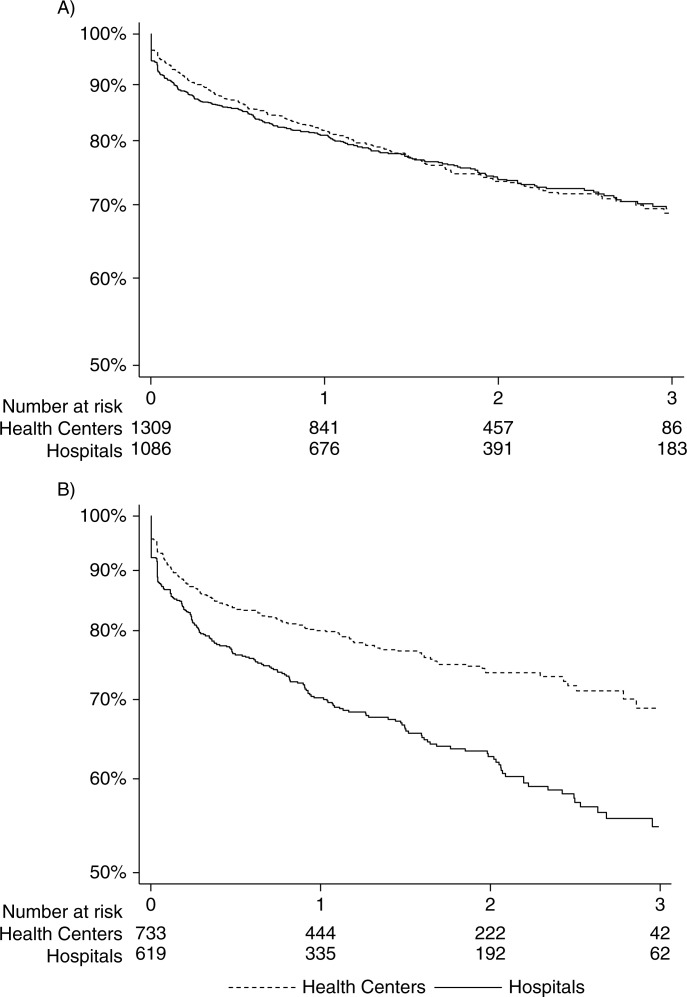
Results: Of 3747 patients, 2042 (54.5%) started ART at HCs. Both women and men at hospitals had more advanced clinical and immunological stages of disease than those at HCs. Over 5445 patient-years, 420 died and 475 were LTFU. Kaplan-Meier estimates for three-year retention were 68.7 and 69.7% at HCs and hospitals, respectively, among women (p=0.81) and 68.8% at HCs versus 54.7% at hospitals among men (p<0.001). These findings persisted in adjusted analyses, with similar retention at HCs and hospitals among women (odds ratio (OR): 0.89, 95% confidence interval (CI): 0.73-1.09) and higher retention at HCs among men (OR: 1.53, 95% CI: 1.20-1.96). The latter result was mainly driven by a lower proportion of patients LTFU at HCs (OR: 0.68, 95% CI: 0.51-0.93).
Conclusions: In rural Lesotho, overall retention in care did not differ significantly between nurse-led HCs and hospitals. However, men seemed to benefit most from starting ART at HCs, as they were more likely to remain in care in these facilities compared to hospitals.
Keywords: HIV; antiretroviral treatment; decentralization; nurse-based care; retention in care; rural Southern Africa; task shifting.
Figures
References
-
- Van Damme W, Kober K, Laga M. The real challenges for scaling up ART in sub-Saharan Africa. AIDS. 2006;20(5):653–6. - PubMed
-
- Kober K, Van Damme W. Scaling up access to antiretroviral treatment in Southern Africa: who will do the job? Lancet. 2004;364(9428):103–7. - PubMed
-
- World Health Organisation, HIV/AIDS Programme. Task shifting to tackle health worker shortages [Internet] 2007. [cited 2013 Aug 12]. Available from: http://www.who.int/healthsystems/task_shifting_booklet.pdf.
-
- Gilks CF, Crowley S, Ekpini R, Gove S, Perriens J, Souteyrand Y, et al. The WHO public-health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet. 2006;368(9534):505–10. - PubMed
-
- Mulamba F, Hirschhorn A, Oser R. Decentralizing antiretroviral treatment services at primary health care facilities: a guide to expanding access and care in resource-limited, generalized HIV epidemic settings. USAID, AIDSTAR-One Project 2010. [Interner]. [cited 2013 Aug 12]. Available from: http://www.aidstar-one.com/sites/default/files/Decentralizing%20ART_Fina....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
