

Association between point-of-care CRP testing and antibiotic prescribing in respiratory tract infections: a systematic review and meta-analysis of primary care studies
- PMID: 24267862
- PMCID: PMC3809432
- DOI: 10.3399/bjgp13X674477
Association between point-of-care CRP testing and antibiotic prescribing in respiratory tract infections: a systematic review and meta-analysis of primary care studies
Abstract
Background: Most patients with respiratory tract infections (RTIs) are prescribed antibiotics in general practice. However, there is little evidence that antibiotics bring any value to the treatment of most RTIs. Point-of-care C-reactive protein testing may reduce antibiotic prescribing.
Aim: To systematically review studies that have examined the association between point-of-care (POC) C-reactive protein testing and antibiotic prescribing for RTIs in general practice.
Design and setting: Systematic review and meta-analysis of randomised controlled trials and observational studies.
Method: MEDLINE(®) and Embase were systematically searched to identify relevant publications. All studies that examined the association between POC C-reactive protein testing and antibiotic prescribing for patients with RTIs were included. Two authors independently screened the search results and extracted data from eligible studies. Dichotomous measures of outcomes were combined using risk ratios (RRs) with 95% confidence intervals (CIs) either by fixed or random-effect models.
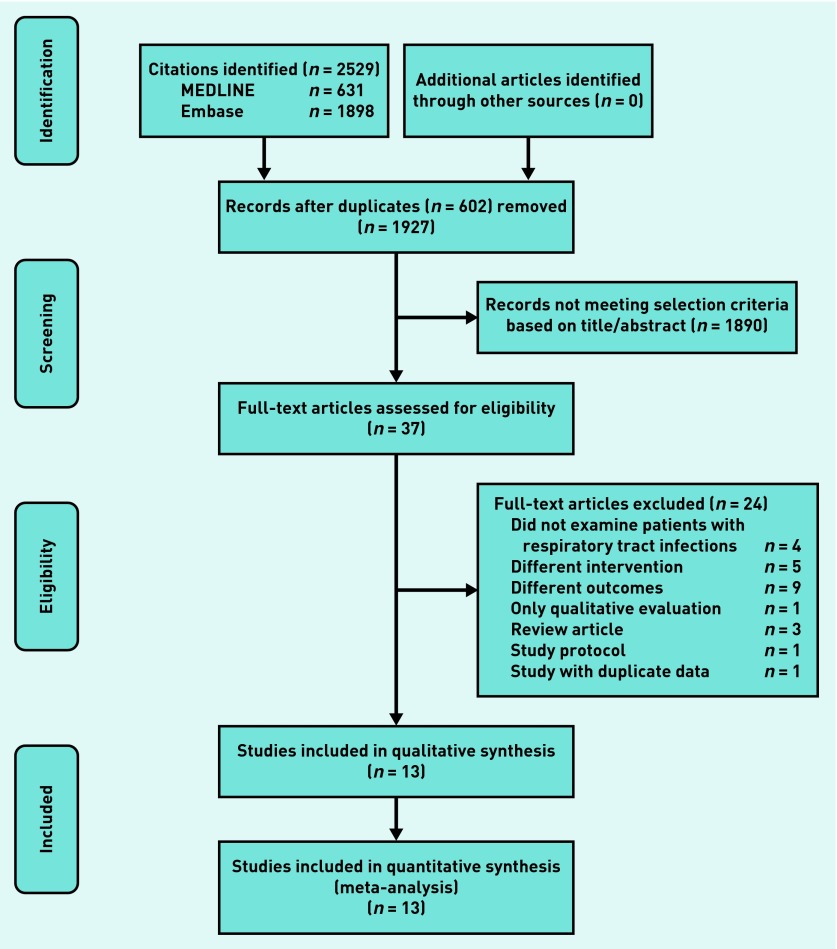
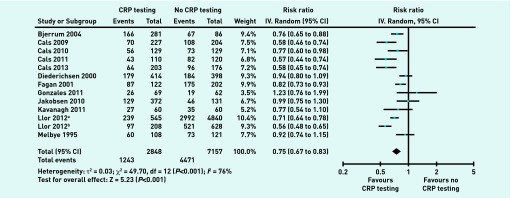
Results: Thirteen studies containing 10 005 patients met the inclusion criteria. POC C-reactive protein testing was associated with a significant reduction in antibiotic prescribing at the index consultation (RR 0.75, 95% CI = 0.67 to 0.83), but was not associated with antibiotic prescribing at any time during the 28-day follow-up period (RR 0.85, 95% CI = 0.70 to 1.01) or with patient satisfaction (RR 1.07, 95% CI = 0.98 to 1.17).
Conclusion: POC C-reactive protein testing significantly reduced antibiotic prescribing at the index consultation for patients with RTIs. Further studies are needed to analyse the confounders that lead to the heterogeneity.
Figures
Comment in
-
Incorrect inclusion of individual studies and methodological flaws in systematic review and meta-analysis.Br J Gen Pract. 2014 May;64(622):221-2. doi: 10.3399/bjgp14X679615. Br J Gen Pract. 2014. PMID: 24771816 Free PMC article. No abstract available.
-
Authors' response.Br J Gen Pract. 2014 May;64(622):222. doi: 10.3399/bjgp14X679624. Br J Gen Pract. 2014. PMID: 24771817 Free PMC article. No abstract available.
References
-
- Thorpe JM, Smith SR, Trygstad TK. Trends in emergency department antibiotic prescribing for acute respiratory tract infections. Ann Pharmacother. 2004;38(6):928–935. - PubMed
-
- Rowbotham S, Chisholm A, Moschogianis S, et al. Challenges to nurse prescribers of a no-antibiotic prescribing strategy for managing self-limiting respiratory tract infections. J Adv Nurs. 2012;68(12):2622–2632. - PubMed
-
- Tan T, Little P, Stokes T, Guideline Development Group Antibiotic prescribing for self limiting respiratory tract infections in primary care: summary of NICE guidance. BMJ. 2008;337:a437. - PubMed
-
- Kotwani A, Wattal C, Katewa S, et al. Factors influencing primary care physicians to prescribe antibiotics in Delhi India. Fam Pract. 2010;27(6):684–690. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous