

Mapping patterns of local recurrence after pancreaticoduodenectomy for pancreatic adenocarcinoma: a new approach to adjuvant radiation field design
- PMID: 24267969
- PMCID: PMC3971882
- DOI: 10.1016/j.ijrobp.2013.09.005
Mapping patterns of local recurrence after pancreaticoduodenectomy for pancreatic adenocarcinoma: a new approach to adjuvant radiation field design
Abstract
Purpose: To generate a map of local recurrences after pancreaticoduodenectomy (PD) for patients with resectable pancreatic ductal adenocarcinoma (PDA) and to model an adjuvant radiation therapy planning treatment volume (PTV) that encompasses a majority of local recurrences.
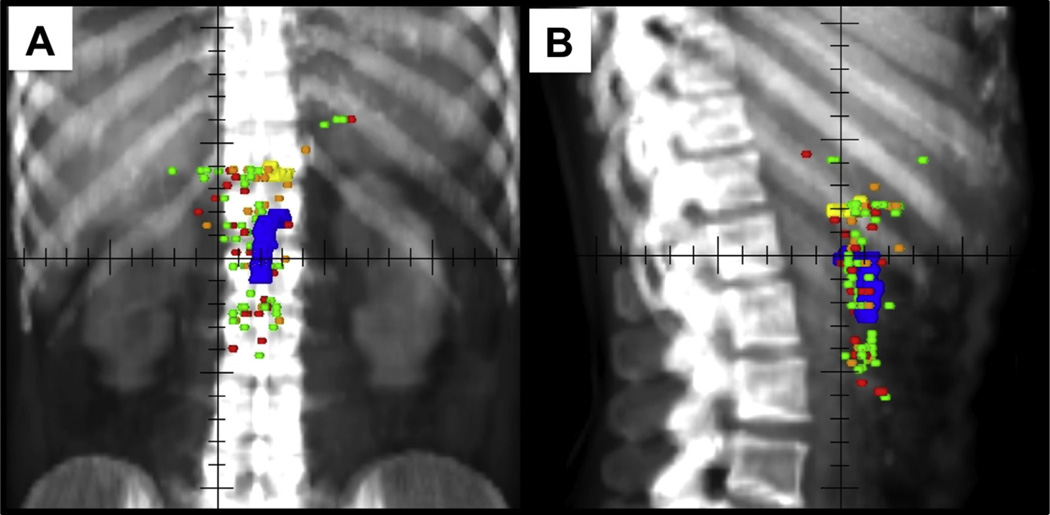
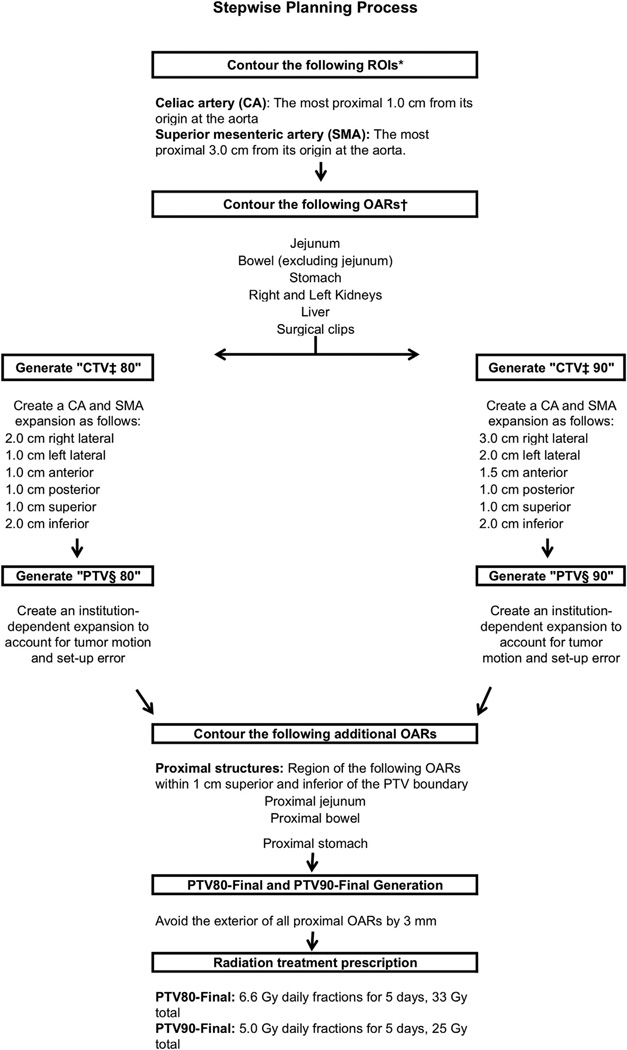
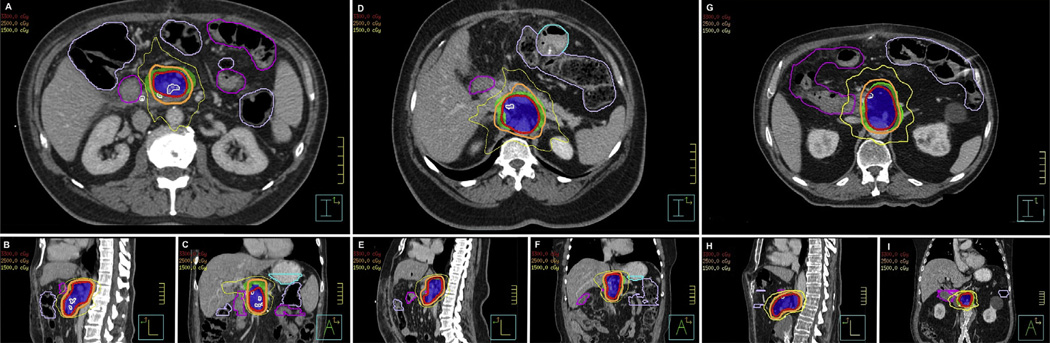
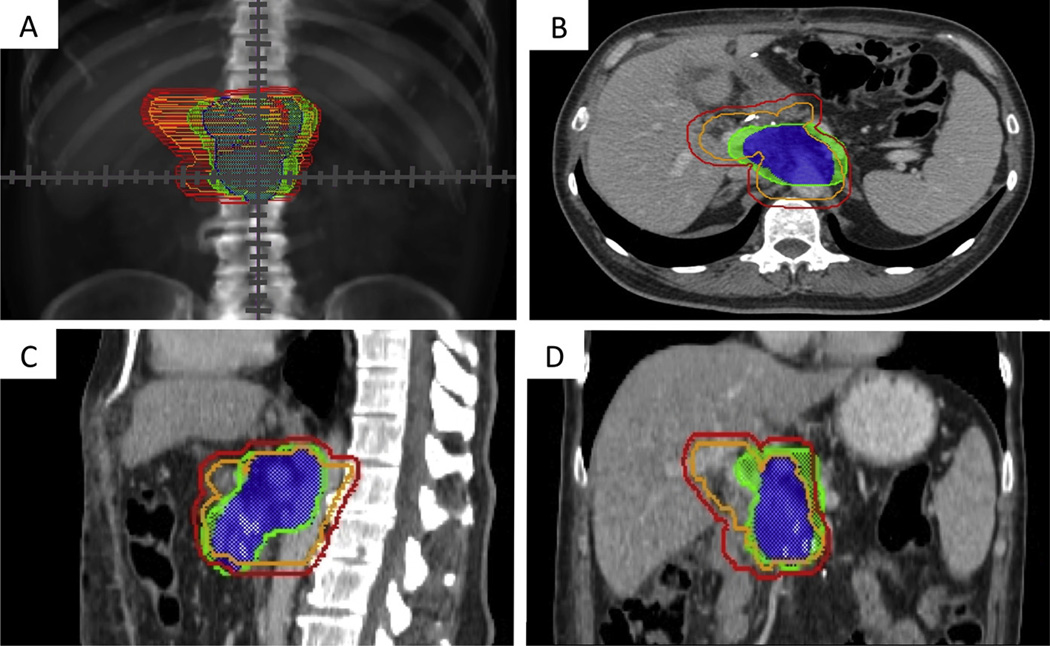
Methods and materials: Consecutive patients with resectable PDA undergoing PD and 1 or more computed tomography (CT) scans more than 60 days after PD at our institution were reviewed. Patients were divided into 3 groups: no adjuvant treatment (NA), chemotherapy alone (CTA), or chemoradiation (CRT). Cross-sectional scans were centrally reviewed, and local recurrences were plotted to scale with respect to the celiac axis (CA), superior mesenteric artery (SMA), and renal veins on 1 CT scan of a template post-PD patient. An adjuvant clinical treatment volume comprising 90% of local failures based on standard expansions of the CA and SMA was created and simulated on 3 post-PD CT scans to assess the feasibility of this planning approach.
Results: Of the 202 patients in the study, 40 (20%), 34 (17%), and 128 (63%) received NA, CTA, and CRT adjuvant therapy, respectively. The rate of margin-positive resections was greater in CRT patients than in CTA patients (28% vs 9%, P=.023). Local recurrence occurred in 90 of the 202 patients overall (45%) and in 19 (48%), 22 (65%), and 49 (38%) in the NA, CTA, and CRT groups, respectively. Ninety percent of recurrences were within a 3.0-cm right-lateral, 2.0-cm left-lateral, 1.5-cm anterior, 1.0-cm posterior, 1.0-cm superior, and 2.0-cm inferior expansion of the combined CA and SMA contours. Three simulated radiation treatment plans using these expansions with adjustments to avoid nearby structures were created to demonstrate the use of this treatment volume.
Conclusions: Modified PTVs targeting high-risk areas may improve local control while minimizing toxicities, allowing dose escalation with intensity-modulated or stereotactic body radiation therapy.
Copyright © 2013 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: none.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- Li D, Xie K, Wolff R, et al. Pancreatic cancer. Lancet. 2004;363:1049–1057. - PubMed
-
- Wagner M, Redaelli C, Lietz M, et al. Curative resection is the single most important factor determining outcome in patients with pancreatic adenocarcinoma. Br J Surg. 2004;91:586–594. - PubMed
-
- Smeenk HG, van Eijck CH, Hop WC, et al. Long-term survival and metastatic pattern of pancreatic and periampullary cancer after adjuvant chemoradiation or observation: Long-term results of EORTC trial 40891. Ann Surg. 2007;246:734–740. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
