

Angiotensin-converting enzyme genetic polymorphism: its impact on cardiac remodeling
- PMID: 24270863
- PMCID: PMC3987401
- DOI: 10.5935/abc.20130229
Angiotensin-converting enzyme genetic polymorphism: its impact on cardiac remodeling
Abstract
Background: The role of angiotensin-converting enzyme genetic polymorphisms as a predictor of echocardiographic outcomes on heart failure is yet to be established. The local profile should be identified so that the impact of those genotypes on the Brazilian population could be identified. This is the first study on exclusively non-ischemic heart failure over a follow-up longer than 5 years.
Objective: To determine the distribution of angiotensin-converting enzyme genetic polymorphism variants and their relation with echocardiographic outcome of patients with non-ischemic heart failure.
Methods: Secondary analysis of the medical records of 111 patients and identification of the angiotensin-converting enzyme genetic polymorphism variants, classified as DD (Deletion/Deletion), DI (Deletion/Insertion) or II (Insertion/Insertion).
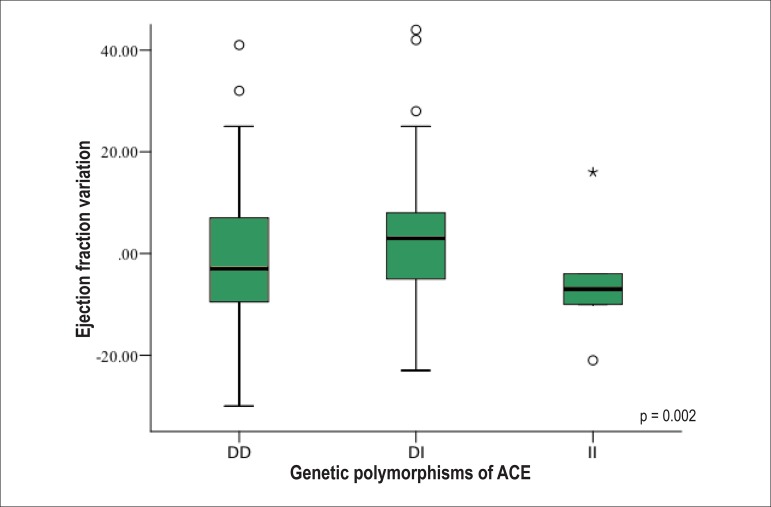
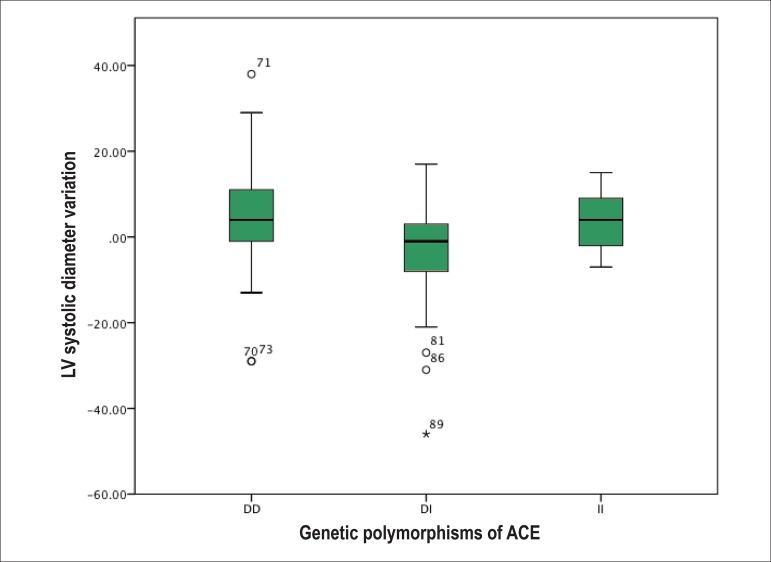
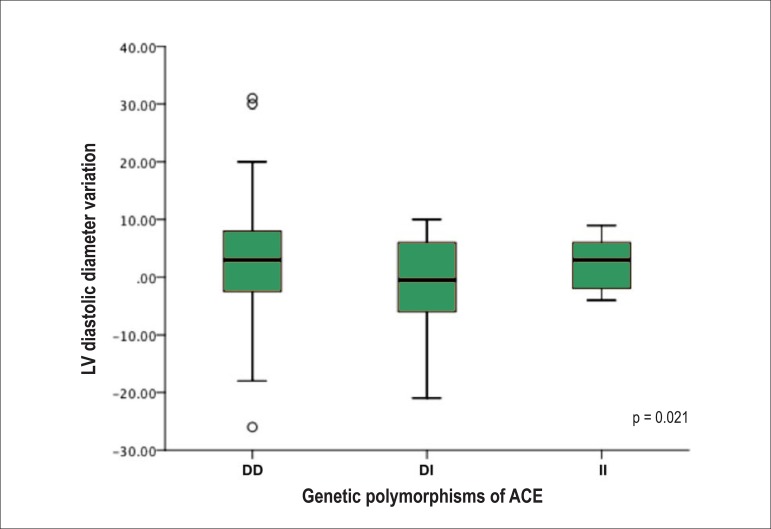
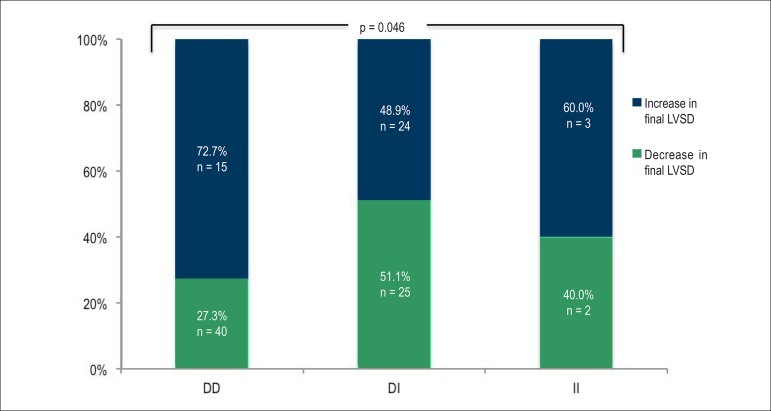
Results: The cohort means were as follows: follow-up, 64.9 months; age, 59.5 years; male sex, 60.4%; white skin color, 51.4%; use of beta-blockers, 98.2%; and use of angiotensin-converting-enzyme inhibitors or angiotensin receptor blocker, 89.2%. The angiotensin-converting enzyme genetic polymorphism distribution was as follows: DD, 51.4%; DI, 44.1%; and II, 4.5%. No difference regarding the clinical characteristics or treatment was observed between the groups. The final left ventricular systolic diameter was the only isolated echocardiographic variable that significantly differed between the angiotensin-converting enzyme genetic polymorphisms: 59.2 ± 1.8 for DD versus 52.3 ± 1.9 for DI versus 59.2 ± 5.2 for II (p = 0.029). Considering the evolutionary behavior, all echocardiographic variables (difference between the left ventricular ejection fraction at the last and first consultation; difference between the left ventricular systolic diameter at the last and first consultation; and difference between the left ventricular diastolic diameter at the last and first consultation) differed between the genotypes (p = 0.024; p = 0.002; and p = 0.021, respectively).
Conclusion: The distribution of the angiotensin-converting enzyme genetic polymorphisms differed from that of other studies with a very small number of II. The DD genotype was independently associated with worse echocardiographic outcome, while the DI genotype, with the best echocardiographic profile (increased left ventricular ejection fraction and decreased left ventricular diameters).
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Angiotensin-converting enzyme genetic polymorphism.Arq Bras Cardiol. 2014 Jun;102(6):611; discussion 611-2. doi: 10.5935/abc.20140077. Arq Bras Cardiol. 2014. PMID: 25004423 Free PMC article. No abstract available.
References
-
- Godoy HL, Silveira JA, Segalla E, Almeida DR. Hospitalização e mortalidade por insuficiência cardíaca em hospitais públicos no município de São Paulo. Arq Bras Cardiol. 2011;97(5):402–407. - PubMed
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127(1):e6–e245. Erratum in: Circulation. 2013;127(1):e841. - PMC - PubMed
-
- Lopes LR, Elliott PM. Genetics of heart failure. Biochim Biophys Acta. 2013 Jan 03; [Epub ahead of print] - PubMed
-
- Bai Y, Wang L, Hu S, Wei Y. Association of angiotensin-converting enzyme I/D polymorphism with heart failure: a meta-analysis. Mol Cell Biochem. 2012;361(1-2):297–304. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
