

Charcot foot in diabetes and an update on imaging
- PMID: 24273635
- PMCID: PMC3837304
- DOI: 10.3402/dfa.v4i0.21884
Charcot foot in diabetes and an update on imaging
Abstract
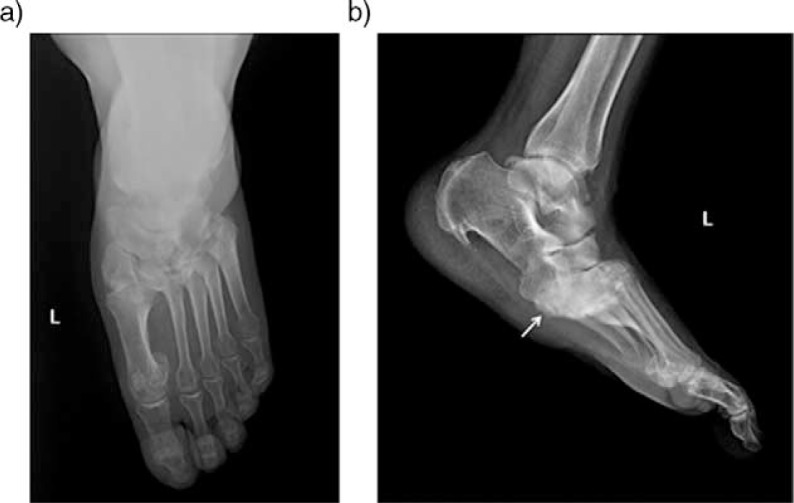
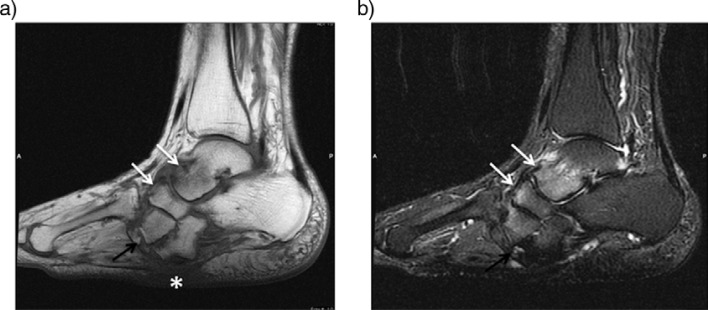
Charcot neuroarthropathy (CN) is a serious complication of diabetes mellitus that can cause major morbidity including limb amputation. Since it was first described in 1883, and attributed to diabetes mellitus in 1936, the diagnosis of CN has been very challenging even for the experienced practitioners. Imaging plays a central role in the early and accurate diagnosis of CN, and in distinction of CN from osteomyelitis. Conventional radiography, computed tomography, nuclear medicine scintigraphy, magnetic resonance imaging, and positron emission tomography are the imaging techniques currently in use for the evaluation of CN but modalities other than magnetic resonance imaging appeared to be complementary. This study focuses on imaging findings of acute and chronic neuropathic osteoarthropathy in diabetes and discrimination of infected vs. non-infected neuropathic osteoarthropathy.
Keywords: Charcot foot; complications; diabetes mellitus; diabetic foot; diagnostic imaging.
Figures



References
-
- Charcot J. Sur quelques arthropathies qui paraissent dependre d'une lesion du cerveau ou de la moelle epiniere. Arch Des Phys Norm Pathol. 1868;1:161.
-
- Malhotra S, Bello E, Kominsky S. Diabetic foot ulcerations: biomechanics, charcot foot, and total contact cast. Semin Vasc Surg. 2012;25:66–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources