

Transluminal endoscopic step-up approach versus minimally invasive surgical step-up approach in patients with infected necrotising pancreatitis (TENSION trial): design and rationale of a randomised controlled multicenter trial [ISRCTN09186711]
- PMID: 24274589
- PMCID: PMC4222267
- DOI: 10.1186/1471-230X-13-161
Transluminal endoscopic step-up approach versus minimally invasive surgical step-up approach in patients with infected necrotising pancreatitis (TENSION trial): design and rationale of a randomised controlled multicenter trial [ISRCTN09186711]
Abstract
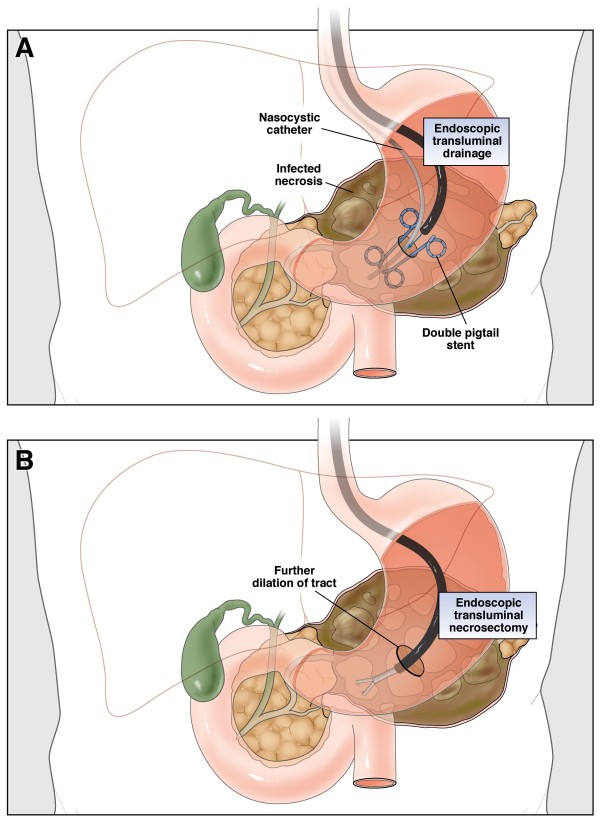
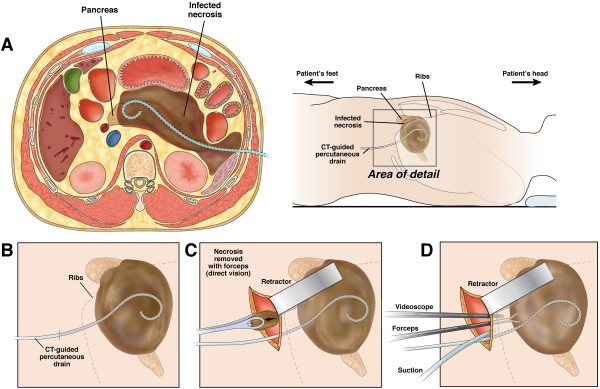
Background: Infected necrotising pancreatitis is a potentially lethal disease that nearly always requires intervention. Traditionally, primary open necrosectomy has been the treatment of choice. In recent years, the surgical step-up approach, consisting of percutaneous catheter drainage followed, if necessary, by (minimally invasive) surgical necrosectomy has become the standard of care. A promising minimally invasive alternative is the endoscopic transluminal step-up approach. This approach consists of endoscopic transluminal drainage followed, if necessary, by endoscopic transluminal necrosectomy. We hypothesise that the less invasive endoscopic step-up approach is superior to the surgical step-up approach in terms of clinical and economic outcomes.
Methods/design: The TENSION trial is a randomised controlled, parallel-group superiority multicenter trial. Patients with (suspected) infected necrotising pancreatitis with an indication for intervention and in whom both treatment modalities are deemed possible, will be randomised to either an endoscopic transluminal or a surgical step-up approach. During a 4 year study period, 98 patients will be enrolled from 24 hospitals of the Dutch Pancreatitis Study Group. The primary endpoint is a composite of death and major complications within 6 months following randomisation. Secondary endpoints include complications such as pancreaticocutaneous fistula, exocrine or endocrine pancreatic insufficiency, need for additional radiological, endoscopic or surgical intervention, the need for necrosectomy after drainage, the number of (re-)interventions, quality of life, and total direct and indirect costs.
Discussion: The TENSION trial will answer the question whether an endoscopic step-up approach reduces the combined primary endpoint of death and major complications, as well as hospital stay and related costs compared with a surgical step-up approach in patients with infected necrotising pancreatitis.
Figures


References
-
- Rodriguez JR, Razo AO, Targarona J, Thayer SP, Rattner DW, Warshaw AL, Fernandez-del Castillo C. Debridement and closed packing for sterile or infected necrotizing pancreatitis: insights into indications and outcomes in 167 patients. Ann Surg. 2008;247(2):294–299. doi: 10.1097/SLA.0b013e31815b6976. - DOI - PMC - PubMed
-
- van Santvoort HC, Besselink MG, Bakker OJ, Hofker HS, Boermeester MA, Dejong CH, van Goor H, Schaapherder AF, van Eijck CH, Bollen TL, van Ramshorst B, Nieuwenhuijs VB, Timmer R, Lameris JS, Kruyt PM, Manusama ER, van der Harst E, van der Schelling GP, Karsten T, Hesselink EJ, van Laarhoven CJ, Rosman C, Bosscha K, de Wit RJ, Houdijk AP, van Leeuwen MS, Buskens E, Gooszen HG. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med. 2010;362(16):1491–1502. doi: 10.1056/NEJMoa0908821. - DOI - PubMed
-
- Besselink MG, van Santvoort HC, Buskens E, Boermeester MA, van Goor H, Timmerman HM, Nieuwenhuijs VB, Bollen TL, van Ramshorst B, Witteman BJ, Rosman C, Ploeg RJ, Brink MA, Schaapherder AF, Dejong CH, Wahab PJ, van Laarhoven CJ, van der Harst E, van Eijck CH, Cuesta MA, Akkermans LM, Gooszen HG. Probiotic prophylaxis in predicted severe acute pancreatitis: a randomised, double-blind, placebo-controlled trial. Lancet. 2008;371(9613):651–659. doi: 10.1016/S0140-6736(08)60207-X. - DOI - PubMed
-
- van Santvoort HC, Bakker OJ, Bollen TL, Besselink MG, Ahmed Ali U, Schrijver AM, Boermeester MA, van Goor H, Dejong CH, van Eijck CH, van Ramshorst B, Schaapherder AF, van der Harst E, Hofker S, Nieuwenhuijs VB, Brink MA, Kruyt PM, Manusama ER, van der Schelling GP, Karsten T, Hesselink EJ, van Laarhoven CJ, Rosman C, Bosscha K, de Wit RJ, Houdijk AP, Cuesta MA, Wahab PJ, Gooszen HG. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology. 2011;141(4):1254–1263. doi: 10.1053/j.gastro.2011.06.073. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
