

Fibrolamellar carcinoma: 2012 update
- PMID: 24278737
- PMCID: PMC3820672
- DOI: 10.6064/2012/743790
Fibrolamellar carcinoma: 2012 update
Abstract
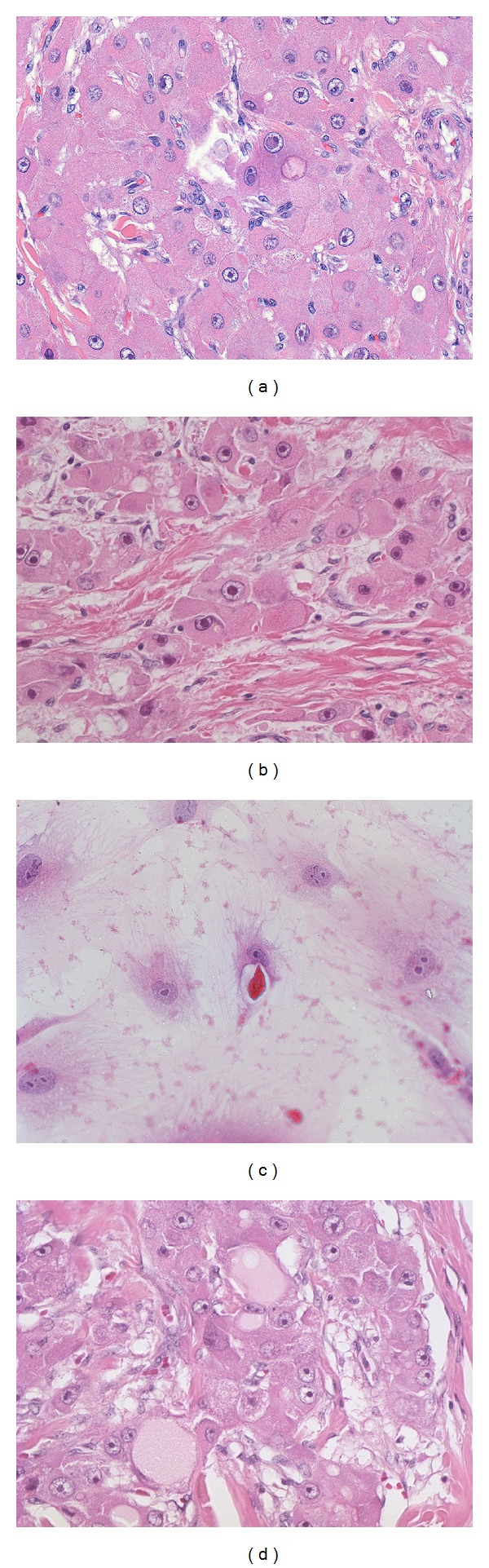
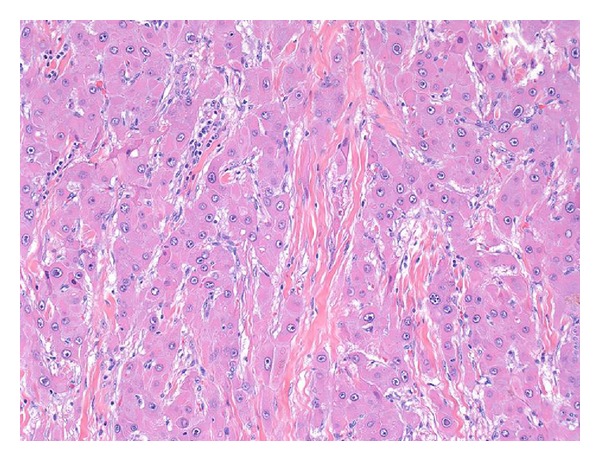
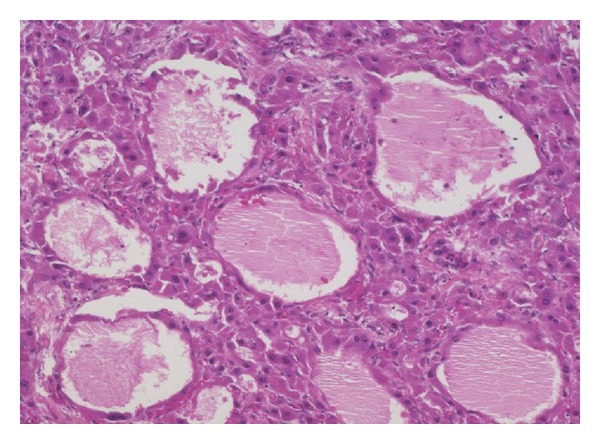
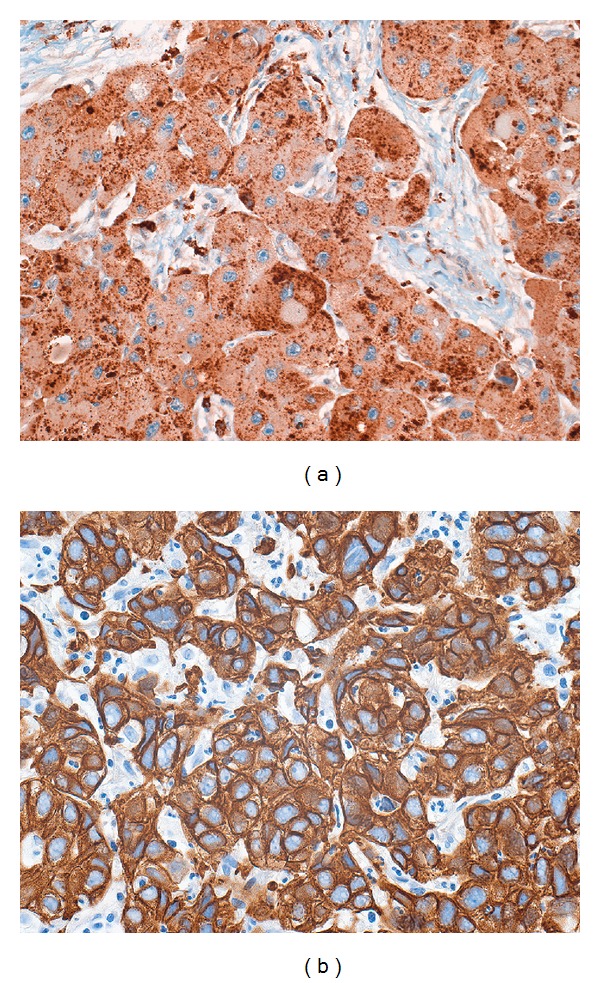
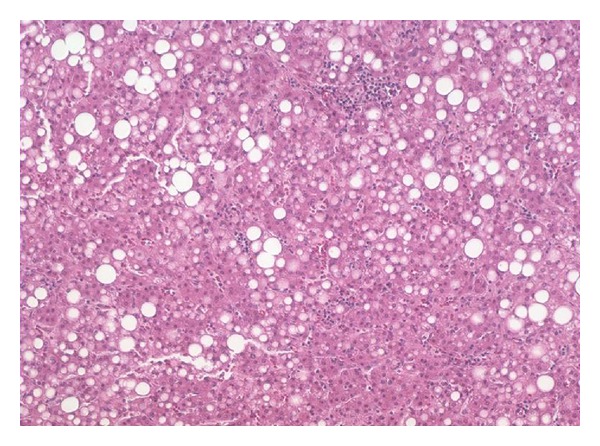
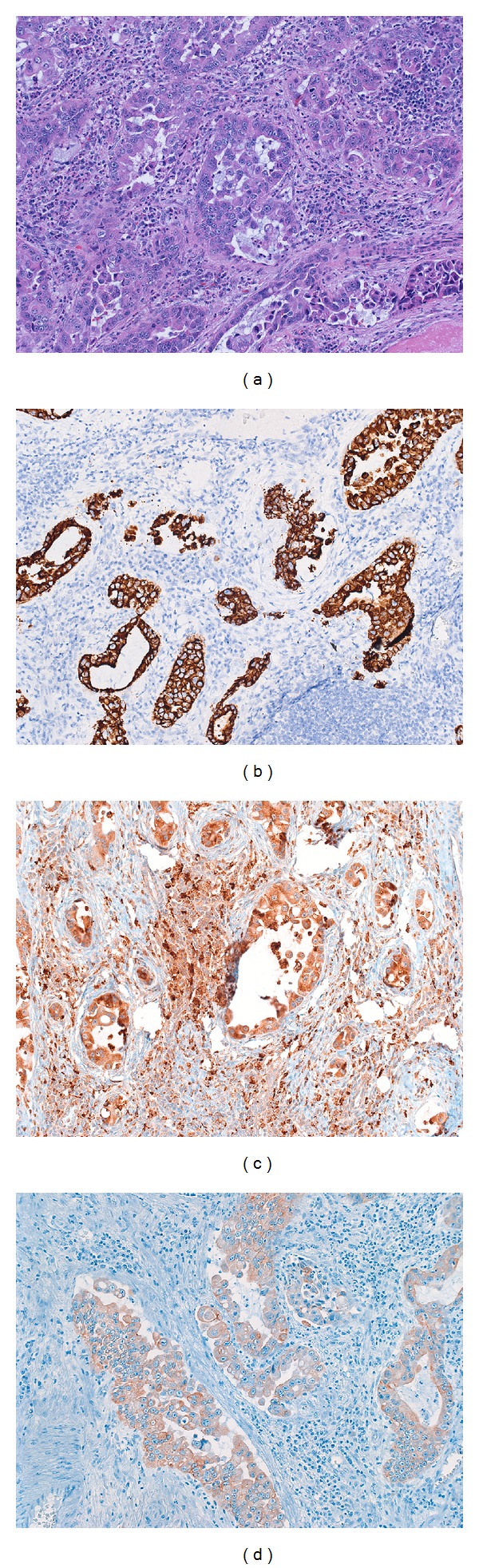
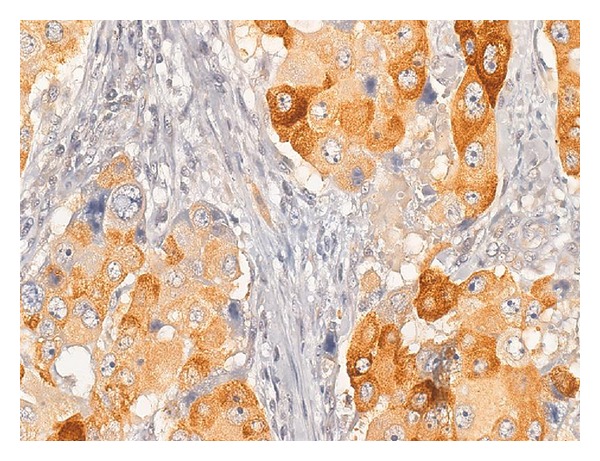
Fibrolamellar carcinomas are a unique type of primary liver cancer. They occur most commonly in children and young adults. Their etiology remains a mystery, as they are not associated with chronic liver disease. Fibrolamellar carcinomas are not indolent tumors, but have an overall better prognosis than typical hepatocellular carcinomas, in part because of the younger age at presentation and the lack of cirrhosis. The most important prognostic feature is whether the tumor is resectable. Histologically, the tumor is made up of large cells that contain abundant mitochondria. The nuclei of the tumor cells have prominent nucleoli. The tumor cells induce the formation of extensive intratumoral fibrosis, which often grows in parallel, or lamellar bands. The tumor cells clearly show hepatocellular features but are also unique in showing both biliary and neuroendocrine differentiation. The uniqueness of fibrolamellar carcinoma extends to their molecular findings. While the genetic abnormalities that lead to fibrolamellar carcinomas are not yet known, studies have shown that they lack mutations in the genes most commonly mutated in typical hepatocellular carcinoma (TP53 and CTNNB1). In this paper, the clinical, pathological, and basic science literature on fibrolamellar carcinoma is comprehensively reviewed. Key areas of needed research are also discussed.
Figures
References
-
- Edmondson HA. Differential diagnosis of tumors and tumor-like lesions of the liver in infancy and childhood. A.M.A. Journal of Diseases of Children. 1956;91(2):168–186. - PubMed
-
- Craig JR, Peters RL, Edmondson HA, Omata M. Fibrolamellar carcinoma of the liver: a tumor of adolescents and young adults with distinctive clinico-pathologic features. Cancer. 1980;46(2):372–379. - PubMed
-
- Torbenson M. Review of the clinicopathologic features of fibrolamellar carcinoma. Advances in Anatomic Pathology. 2007;14(3):217–223. - PubMed
-
- Liu S, Chan KW, Wang B, Qiao L. Fibrolamellar hepatocellular carcinoma. American Journal of Gastroenterology. 2009;104(10):2617–2625. - PubMed
-
- Ward SC, Waxman S. Fibrolamellar carcinoma: a review with focus on genetics and comparison to other malignant primary liver tumors. Seminars in Liver Disease. 2011;31(1):61–70. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
