

Immune-mediated adverse events associated with ipilimumab ctla-4 blockade therapy: the underlying mechanisms and clinical management
- PMID: 24278787
- PMCID: PMC3820355
- DOI: 10.1155/2013/857519
Immune-mediated adverse events associated with ipilimumab ctla-4 blockade therapy: the underlying mechanisms and clinical management
Abstract
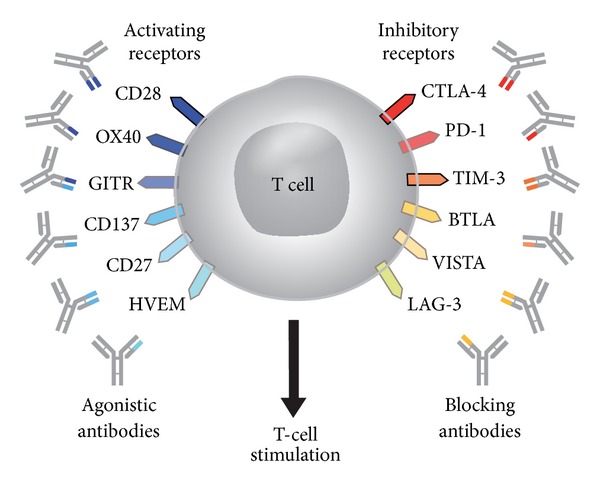
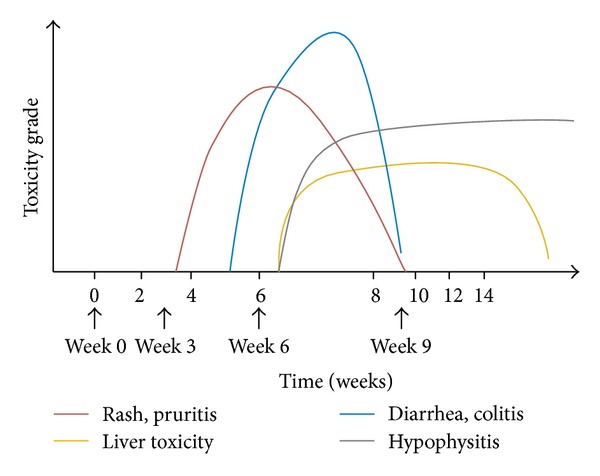
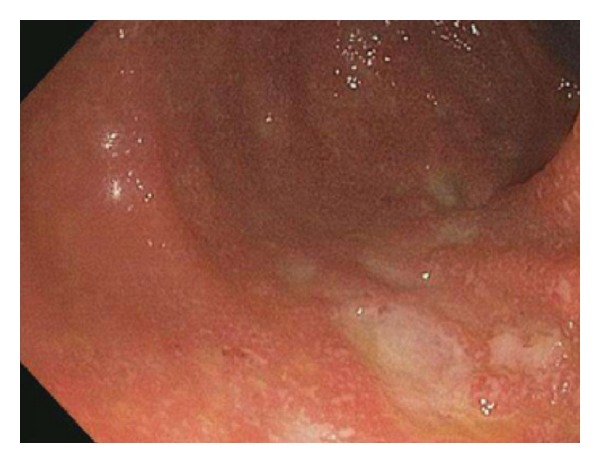
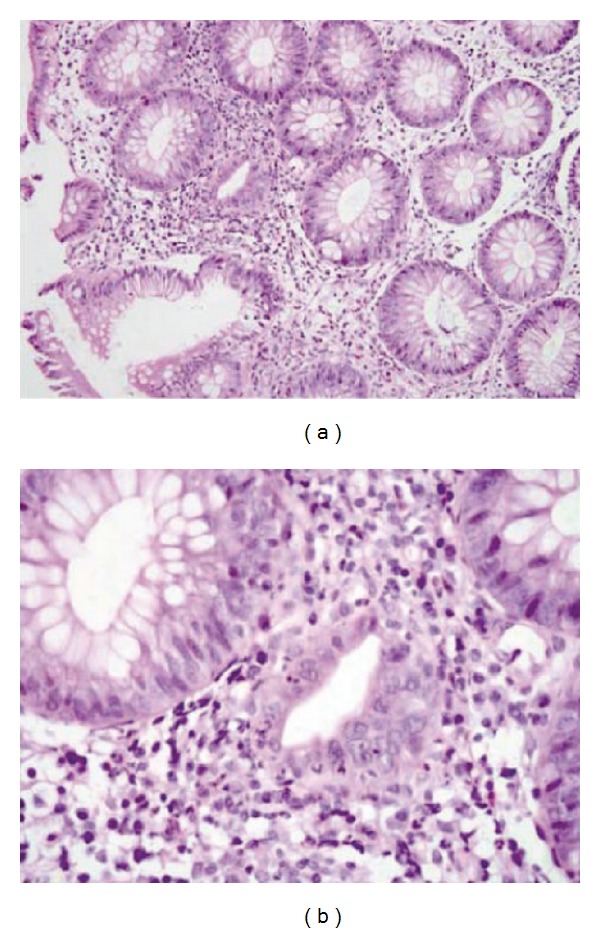
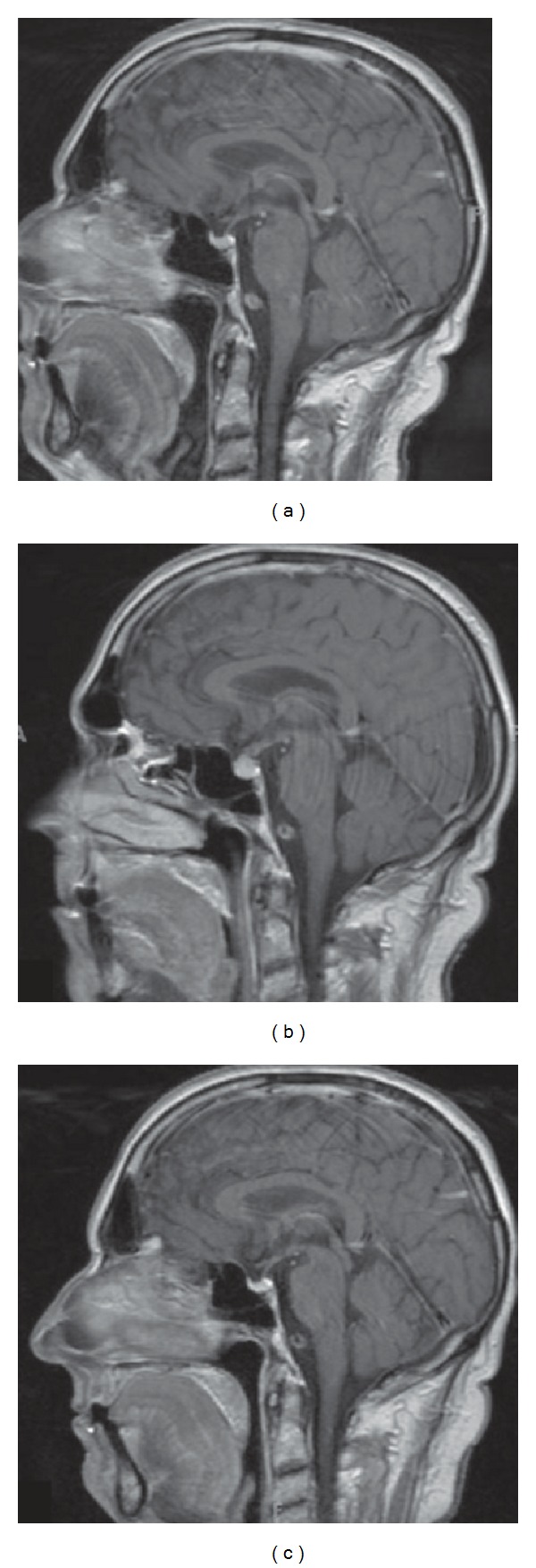
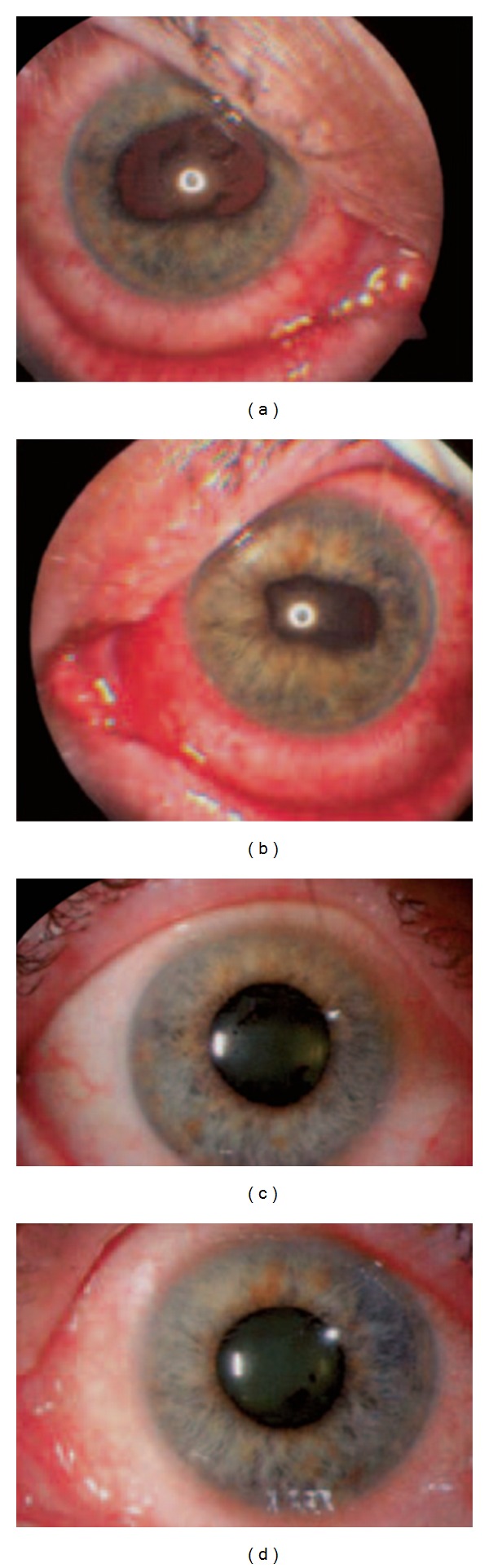
Immunomodulation with the anti-CTLA-4 monoclonal antibody ipilimumab has been shown to extend overall survival (OS) in previously treated and treatment-naive patients with unresectable stage III or IV melanoma. Blockade of CTLA-4 signaling with ipilimumab prolongs T-cell activation and restores T-cell proliferation, thus amplifying T-cell-mediated immunity and the patient's capacity to mount an effective antitumor immune response. While this immunostimulation has unprecedented OS benefits in the melanoma setting, it can also result in immune-mediated effects on various organ systems, leading to immune-related adverse events (irAEs). Ipilimumab-associated irAEs are common and typically low grade and manageable, but can also be serious and life threatening. The skin and gastrointestinal tract are most frequently affected, while hepatic, endocrine, and neurologic events are less common. With proper management, most irAEs resolve within a relatively short time, with a predictable resolution pattern. Prompt and appropriate management of these irAEs is essential and treatment guidelines have been developed to assist oncologists and their teams. Implementation of these irAE management algorithms will help ensure that patients are able to benefit from ipilimumab therapy with adequate control of toxicities.
Figures
References
-
- Sznol M. Betting on immunotherapy for melanoma. Current Oncology Reports. 2009;11(5):397–404. - PubMed
-
- Komenaka I, Hoerig H, Kaufman HL. Immunotherapy for melanoma. Clinics in Dermatology. 2004;22(3):251–265. - PubMed
-
- Gogas H, Ioannovich J, Dafni U, et al. Prognostic significance of autoimmunity during treatment of melanoma with interferon. The New England Journal of Medicine. 2006;354(7):709–718. - PubMed
-
- Clemente CG, Mihm MC, Jr., Bufalino R, Zurrida S, Collini P, Cascinelli N. Prognostic value of tumor infiltrating lymphocytes in the vertical growth phase of primary cutaneous melanoma. Cancer. 1996;77(7):1303–1310. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
