

Intraperitoneal dedifferentiated liposarcoma showing MDM2 amplification: case report
- PMID: 24279301
- PMCID: PMC4222875
- DOI: 10.1186/1477-7819-11-305
Intraperitoneal dedifferentiated liposarcoma showing MDM2 amplification: case report
Abstract
Background: Liposarcoma is the most common type of soft tissue sarcoma (STS). It is divided into five groups according to histological pattern: well-differentiated, myxoid, round cell, pleomorphic, and dedifferentiated. Dedifferentiated liposarcoma most commonly occurs in the retroperitoneum, while an intraperitoneal location is extremely rare. Only seven cases have been reported in literature. Many pathologists recognize that a large number of intra-abdominal poorly differentiated sarcomas are dedifferentiated liposarcomas. We report a case initially diagnosed as undifferentiated sarcoma that was reclassified as intraperitoneal dedifferentiated liposarcoma showing an amplification of the MDM2 gene.
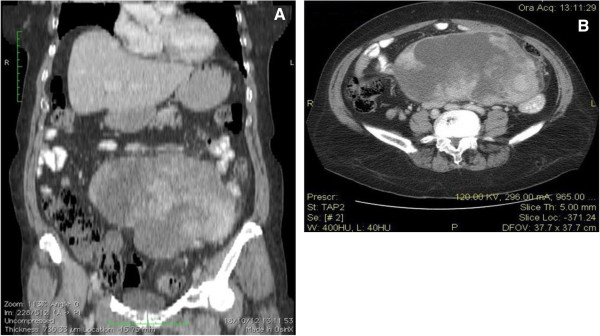
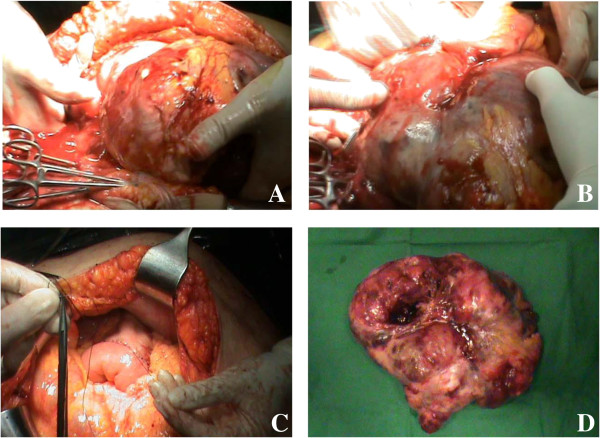
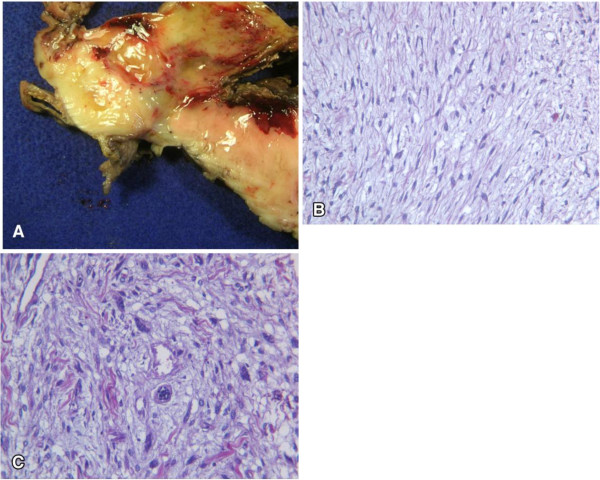
Case presentation: A 59-year-old woman with abdominal pain and constipation was referred to the Department of Advanced Biomedical Sciences, University of Naples Federico II, Naples, Italy, in November 2012. On physical examination, a very large firm mass was palpable in the meso-hypogastrium. Computed tomography (CT) scan showed a heterogeneous density mass (measuring 10 × 19 cm) that was contiguous with the mesentery and compressed the third part of the duodenum and jejunum.At laparotomy, a large mass occupying the entire abdomen was found, adhering to the first jejunal loop and involving the mesentery. Surgical removal of the tumor along with a jejunal resection was performed because the first jejunal loop was firmly attached to the tumor.Macroscopic examination showed a solid, whitish, cerebroid, and myxoid mass, with variable hemorrhage and cystic degeneration, measuring 26 × 19 × 5 cm. Microscopic examination revealed two main different morphologic patterns: areas with spindle cells in a myxoid matrix and areas with pleomorphic cells. The case was initially diagnosed as undifferentiated pleomorphic sarcoma. Histological review showed areas of well-differentiated liposarcoma. Fluorescence in situ hybridization (FISH) analysis was performed and demonstrated an amplification of the MDM2 gene. Definitive diagnosis was intraperitoneal dedifferentiated liposarcoma.No adjuvant therapy was given, but 5 months after laparotomy, the patient presented with a locoregional recurrence and chemotherapy with high-dose ifosfamide was started.
Conclusions: No guidelines are available for the management of intraperitoneal dedifferentiated liposarcoma. We report this case to permit the collection of a larger number of cases to improve understanding and management of this tumor. Moreover, this study strongly suggests that poorly differentiated sarcomas should prompt extensive sampling to demonstrate a well-differentiated liposarcoma component and, if possible, FISH analysis.
Figures
References
-
- Capasso L, Carlomagno N, De Vita F, Orditura M, Paternoster M, Catalano G, Renda A. Leiomyosarcoma of the small intestines: case reports. Ann Ital Chir. 1997;68(6):845–850. - PubMed
-
- Carlomagno N, Dodaro C, Boccia L, Mazzarella L, Renda A. Desmoid tumors of the abdominal wall. G Chir. 1992;13(5):312–314. - PubMed
-
- Enzinger FM, Weiss SW. In: Enzinger and Weiss’sSoft Tissue Tumors. 5th edition. Enzinger FM, Weiss SW, editor. St Louis, MO: Mosby; 2008. Liposarcoma; pp. 477–516.
-
- Weidner N, Cote RJ, Suster S, Weiss MD. Modern Surgical Pathology. 2nd edition. Philadelphia. PA: Saunders; 2009.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
