

Patient preferences for surgical versus medical therapy for ulcerative colitis
- PMID: 24280881
- PMCID: PMC4137889
- DOI: 10.1097/01.MIB.0000437498.14804.50
Patient preferences for surgical versus medical therapy for ulcerative colitis
Abstract
Background: Therapy options for mesalamine-refractory ulcerative colitis (UC) include immunosuppressive medications or surgery. Chronic immunosuppressive therapy increases risks of infection and cancer, whereas surgery produces a permanent change in bowel function. We sought to quantify the willingness of patients with UC to accept the risks of chronic immunosuppression to avoid colectomy.
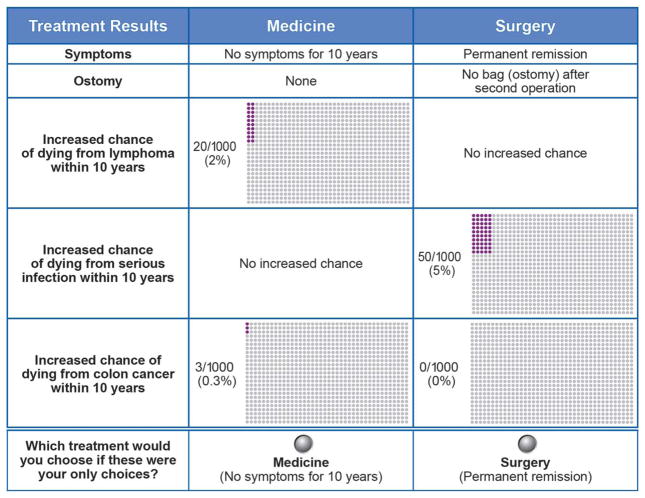
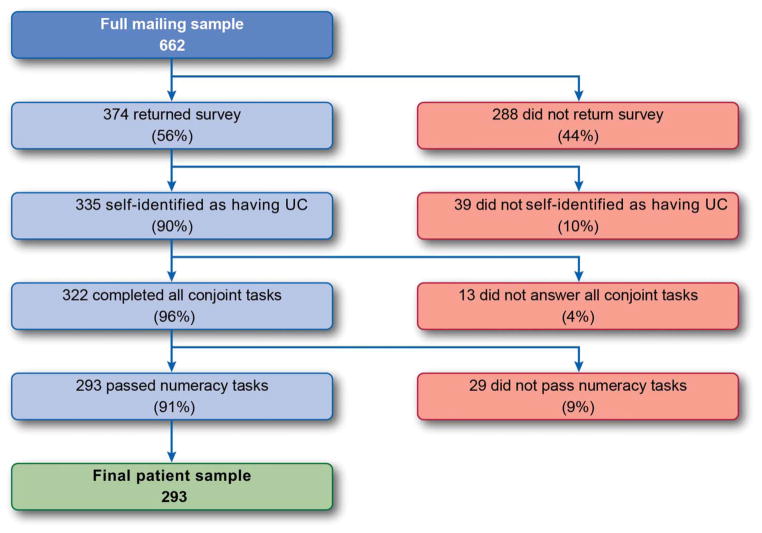
Methods: We conducted a state-of-the-art discrete-choice experiment among 293 patients with UC who were offered a choice of medication or surgical treatments with different features. Random parameters logit was used to estimate patients' willingness to accept trade-offs among treatment features in selecting surgery versus medical treatment.
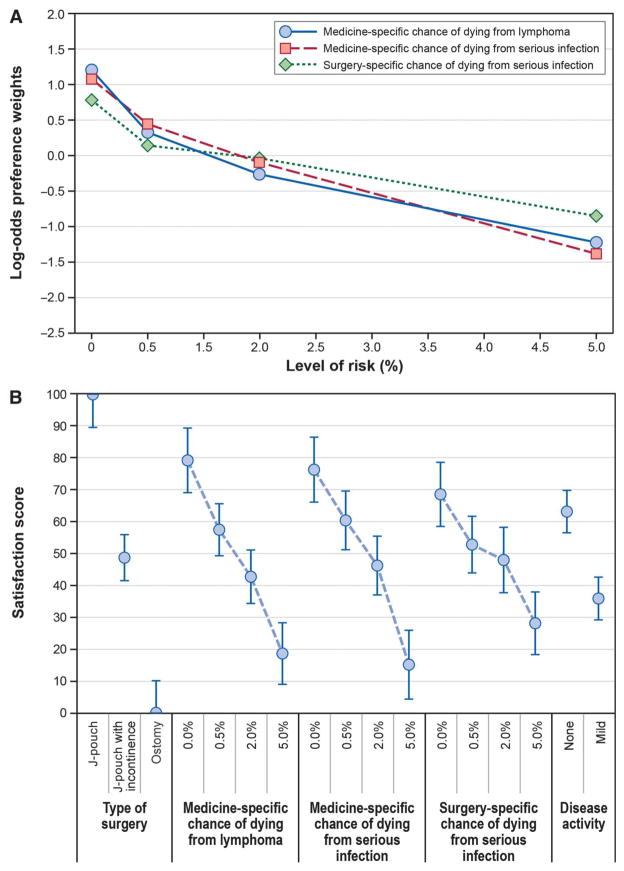
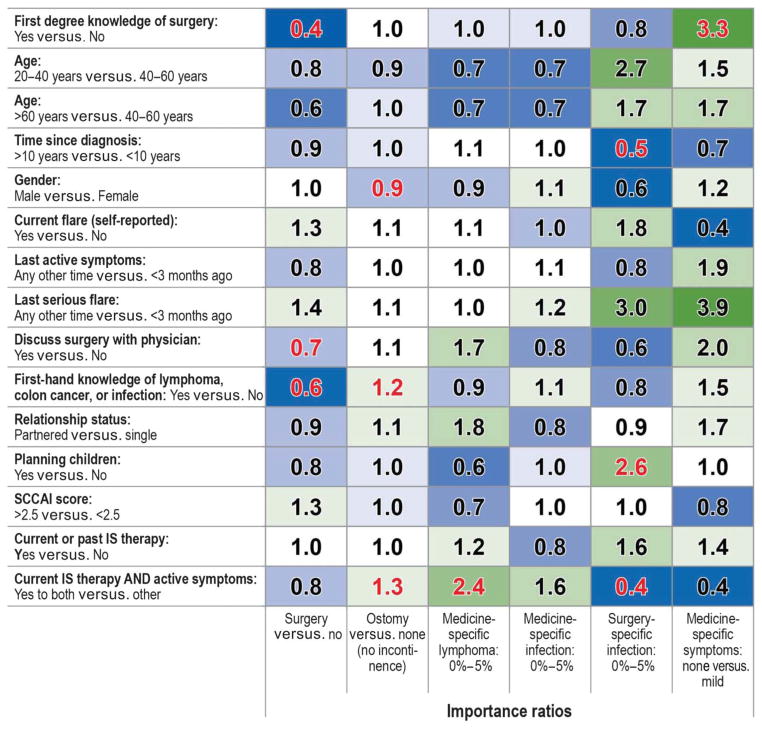
Results: A desire to avoid surgery and the surgery type (ostomy versus J-pouch) influenced patients' choices more than a specified range of 10-year mortality risks from lymphoma or infection, or disease activity (mild versus remission). To avoid an ostomy, patients were willing to accept a >5% 10-year risk of dying from lymphoma or infection from medical therapy, regardless of medication efficacy. However, data on patients' stated choice indicated perceived equivalence between J-pouch surgery and incompletely effective medical therapy. Patient characteristics and disease history influenced patients' preferences regarding surgery versus medical therapy.
Conclusions: Patients with UC are willing to accept relatively high risks of fatal complications from medical therapy to avoid a permanent ostomy and to achieve durable clinical remission. However, patients view J-pouch surgery, but not permanent ileostomy, as an acceptable therapy for refractory UC in which medical therapy is unable to induce a durable remission.
Figures
References
-
- Su C, Lewis JD, Goldberg B, et al. A meta-analysis of the placebo rates of remission and response in clinical trials of active ulcerative colitis. Gastroenterology. 2007;132:516–526. - PubMed
-
- Timmer A, McDonald JW, Macdonald JK. Azathioprine and 6-mercaptopurine for maintenance of remission in ulcerative colitis. Cochrane Database Syst Rev. 2007;9:CD000478. - PubMed
-
- Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353:2462–2476. - PubMed
-
- Toruner M, Loftus EV, Jr, Harmsen WS, et al. Risk factors for opportunistic infections in patients with inflammatory bowel disease. Gastroenterology. 2008;134:929–936. - PubMed
-
- Lewis JD, Gelfand JM, Troxel AB, et al. Immunosuppressant medications and mortality in inflammatory bowel disease. Am J Gastroenterol. 2008;103:1428–1435. quiz 1436. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
