

Testosterone dose-response relationships in hysterectomized women with or without oophorectomy: effects on sexual function, body composition, muscle performance and physical function in a randomized trial
- PMID: 24281237
- PMCID: PMC4701202
- DOI: 10.1097/GME.0000000000000093
Testosterone dose-response relationships in hysterectomized women with or without oophorectomy: effects on sexual function, body composition, muscle performance and physical function in a randomized trial
Abstract
Objective: This study aims to determine the dose-dependent effects of testosterone on sexual function, body composition, muscle performance, and physical function in hysterectomized women with or without oophorectomy.
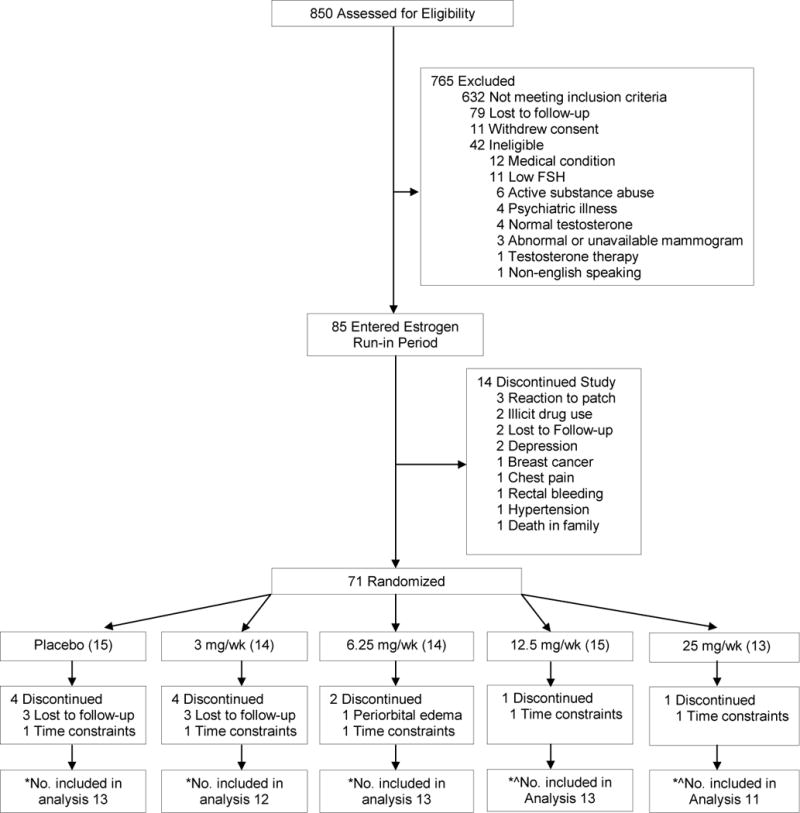
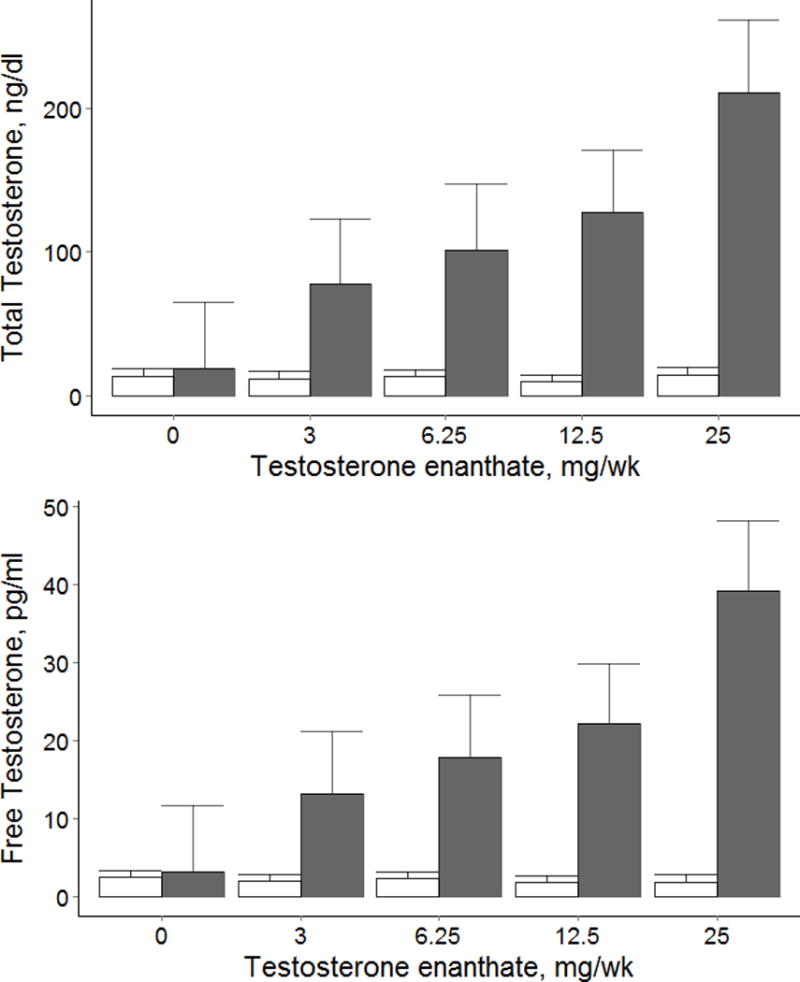
Methods: Seventy-one postmenopausal women who previously underwent hysterectomy with or without oophorectomy and had total testosterone levels less than 31 ng/dL or free testosterone levels less than 3.5 pg/mL received a standardized transdermal estradiol regimen during the 12-week run-in period and were randomized to receive weekly intramuscular injections of placebo or 3, 6.25, 12.5, or 25 mg of testosterone enanthate for 24 weeks. Total and free testosterone levels were measured by liquid chromatography-tandem mass spectrometry and equilibrium dialysis, respectively. The primary outcome was change in sexual function measured by the Brief Index of Sexual Functioning for Women. Secondary outcomes included changes in sexual activity, sexual distress, Derogatis Interview for Sexual Functioning, lean body mass, fat mass, muscle strength and power, and physical function.
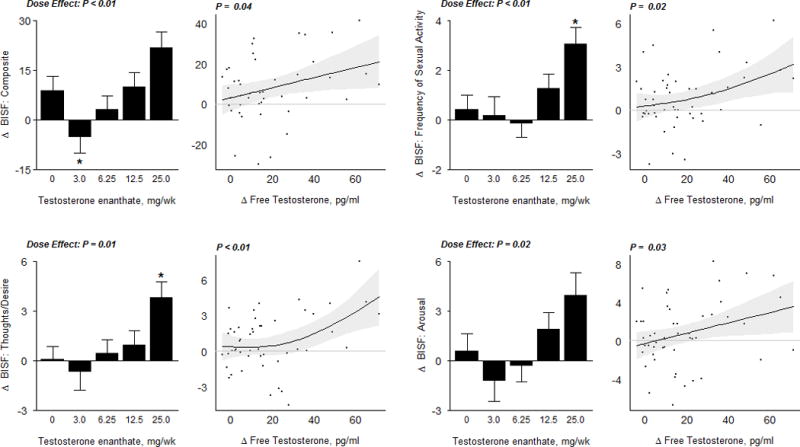
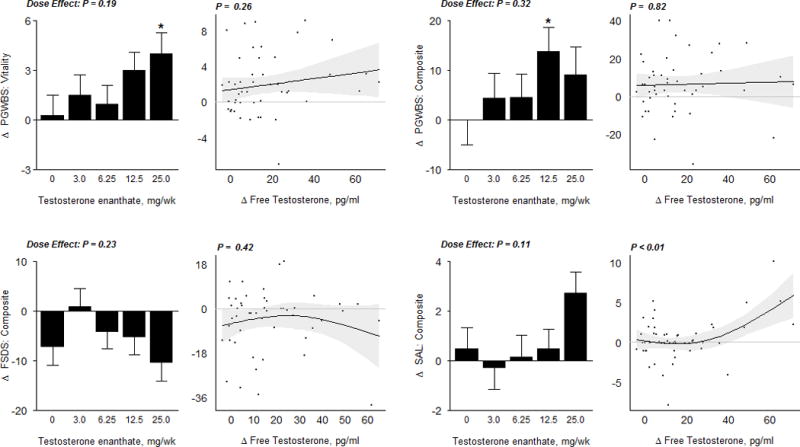
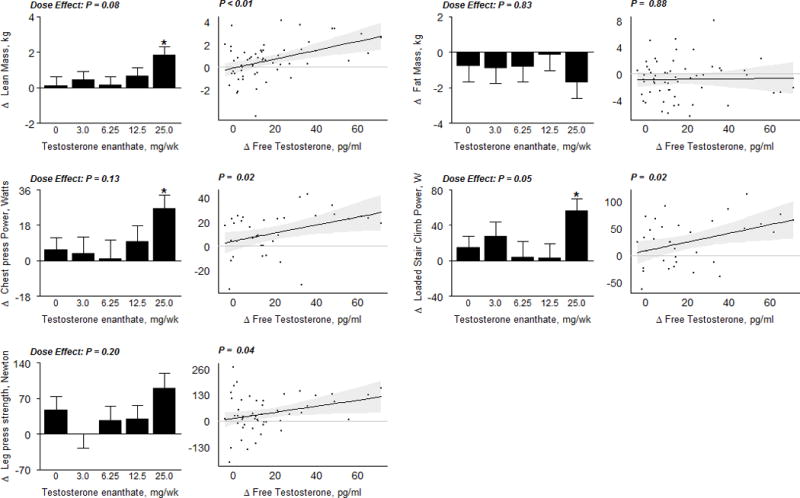
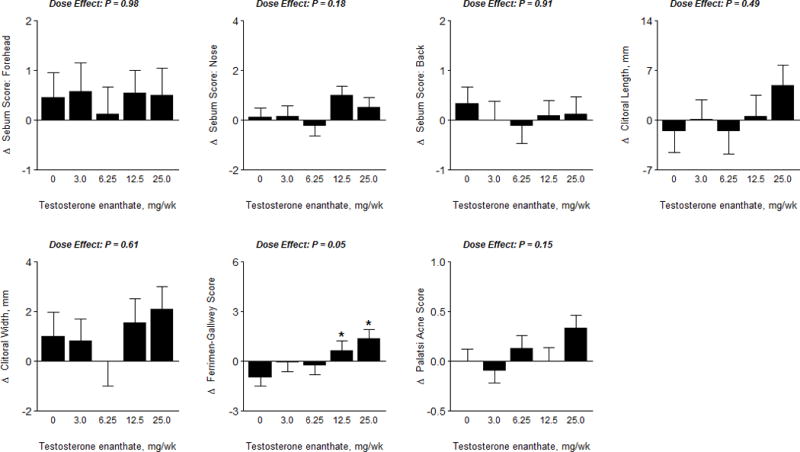
Results: Seventy-one women were randomized; five groups were similar at baseline. Sixty-two women with analyzable data for the primary outcome were included in the final analysis. The mean on-treatment total testosterone concentrations were 19, 78, 102, 128, and 210 ng/dL in the placebo, 3-mg, 6.25-mg, 12.5-mg, and 25-mg groups, respectively. Changes in composite Brief Index of Sexual Functioning for Women scores, thoughts/desire, arousal, frequency of sexual activity, lean body mass, chest-press power, and loaded stair-climb power were significantly related to increases in free testosterone concentrations; compared with placebo, changes were significantly greater in women assigned to the 25-mg group, but not in women in the lower-dose groups. Sexual activity increased by 2.7 encounters per week in the 25-mg group. The frequency of androgenic adverse events was low.
Conclusions: Testosterone administration in hysterectomized women with or without oophorectomy for 24 weeks was associated with dose and concentration-dependent gains in several domains of sexual function, lean body mass, chest-press power, and loaded stair-climb power. Long-term trials are needed to weigh improvements in these outcomes against potential long-term adverse effects.
Trial registration: ClinicalTrials.gov NCT00494208.
Conflict of interest statement
Figures
References
-
- Padero MC, Bhasin S, Friedman TC. Androgen supplementation in older women: too much hype, not enough data. Journal of the American Geriatrics Society. 2002;50(6):1131–40. - PubMed
-
- Basaria S, Dobs AS. Clinical review: Controversies regarding transdermal androgen therapy in postmenopausal women. The Journal of Clinical Endocrinology and Metabolism. 2006;91(12):4743–52. - PubMed
-
- Laughlin GA, Barrett-Connor E, Kritz-Silverstein D, von Muhlen D. Hysterectomy, oophorectomy, and endogenous sex hormone levels in older women: the Rancho Bernardo Study. The Journal of Clinical Endocrinology and Metabolism. 2000;85(2):645–51. - PubMed
-
- Maserejian NN, Shifren J, Parish SJ, Segraves RT, Huang L, Rosen RC. Sexual arousal and lubrication problems in women with clinically diagnosed hypoactive sexual desire disorder: preliminary findings from the hypoactive sexual desire disorder registry for women. Journal of Sex & Marital Therapy. 2012;38(1):41–62. - PubMed
-
- Zussman L, Zussman S, Sunley R, Bjornson E. Sexual response after hysterectomy-oophorectomy: recent studies and reconsideration of psychogenesis. American Journal of Obstetrics and Gynecology. 1981;140(7):725–9. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
