

Clinical course of atrial fibrillation in older adults: the importance of cardiovascular events beyond stroke
- PMID: 24282186
- PMCID: PMC3896863
- DOI: 10.1093/eurheartj/eht483
Clinical course of atrial fibrillation in older adults: the importance of cardiovascular events beyond stroke
Abstract
Aims: Atrial fibrillation increases the risks of stroke, heart failure, and death, and anticoagulation therapy increases the risk of gastrointestinal haemorrhage. However, the relative event rates for these outcomes are not well described. We sought to define the risks of major clinical events in older adults after a new diagnosis of atrial fibrillation.
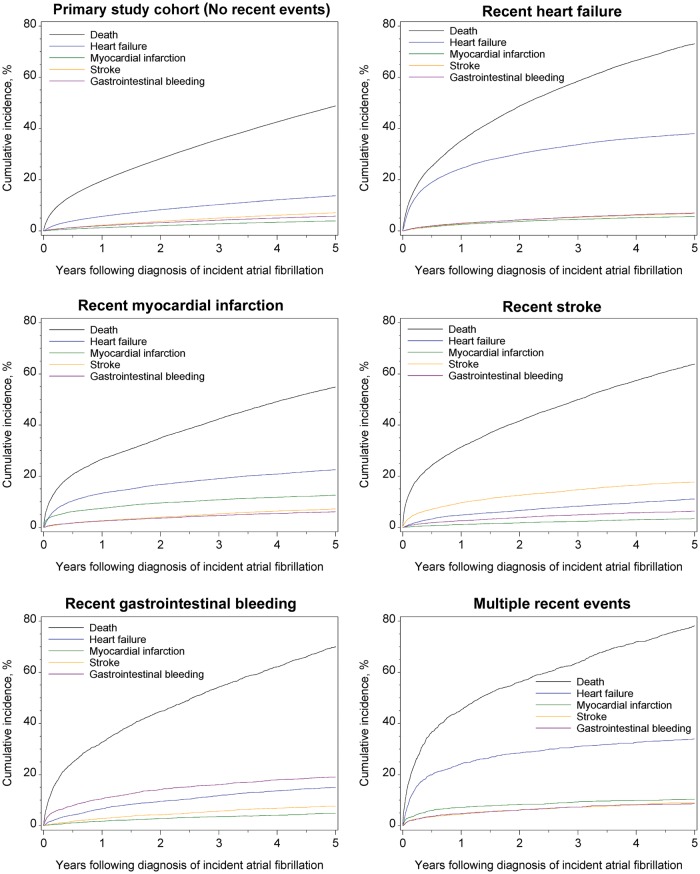
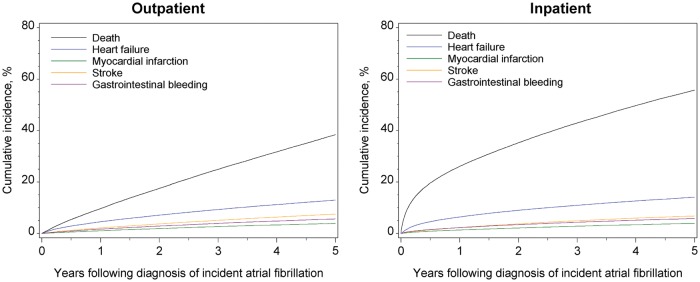
Methods and results: We undertook a population-based, retrospective cohort study of a nationally representative sample of fee-for-service Medicare beneficiaries 65 years or older with incident atrial fibrillation diagnosed between 1999 and 2007. The main outcome measures were mortality and hospitalization or emergency department care for heart failure, myocardial infarction, stroke, or gastrointestinal haemorrhage. Among 186 461 patients with atrial fibrillation and no recent hospitalizations for heart failure, myocardial infarction, stroke, or gastrointestinal haemorrhage, mortality was the most frequent of these major clinical events (19.5% at 1 year; 48.8% at 5 years). By 5 years, 13.7% of patients were hospitalized for heart failure, 7.1% developed new-onset stroke, and 5.7% had gastrointestinal haemorrhage. Myocardial infarction was less frequent (3.9% at 5 years). Rates of mortality, heart failure, myocardial infarction, stroke, and gastrointestinal bleeding increased with older age and higher CHADS2 scores. Among 44 479 patients with previous events, the 5-year risk of death was greatest among patients with recent bleeding events (70.1%) and stroke (63.7%) and lowest among those with recent myocardial infarction (54.9%).
Conclusion: After the diagnosis of incident atrial fibrillation in older adults, mortality was the most frequent major outcome during the first 5 years. Among non-fatal cardiovascular events, heart failure was the most common event.
Keywords: Atrial fibrillation; Heart failure; Mortality; Outcome assessment (health care).
Figures
References
-
- Piccini JP, Hammill BG, Sinner MF, Jensen PN, Hernandez AF, Heckbert SR, Benjamin EJ, Curtis LH. Incidence and prevalence of atrial fibrillation and associated mortality among Medicare beneficiaries, 1993–2007. Circ Cardiovasc Qual Outcomes. 2012;5:85–93. doi:10.1161/CIRCOUTCOMES.111.962688. - DOI - PMC - PubMed
-
- Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med. 2002;113:359–364. doi:10.1016/S0002-9343(02)01236-6. - DOI - PubMed
-
- Institute of Medicine. Initial National Priorities for Comparative Effectiveness Research. Washington, DC: National Academies Press; 2009. http://www.nap.edu/openbook.php?record_id=12648 8 August 2012.
-
- Quan H, Sundararajan V, Halfon P, Fong A, Burnand B, Luthi JC, Saunders LD, Beck CA, Feasby TE, Ghali WA. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43:1130–1139. doi:10.1097/01.mlr.0000182534.19832.83. - DOI - PubMed
-
- Birman-Deych E, Waterman AD, Yan Y, Nilasena DS, Radford MJ, Gage BF. Accuracy of ICD-9-CM codes for identifying cardiovascular and stroke risk factors. Med Care. 2005;43:480–485. doi:10.1097/01.mlr.0000160417.39497.a9. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
