

Rare cystic liver lesions: a diagnostic and managing challenge
- PMID: 24282350
- PMCID: PMC3837259
- DOI: 10.3748/wjg.v19.i43.7603
Rare cystic liver lesions: a diagnostic and managing challenge
Abstract
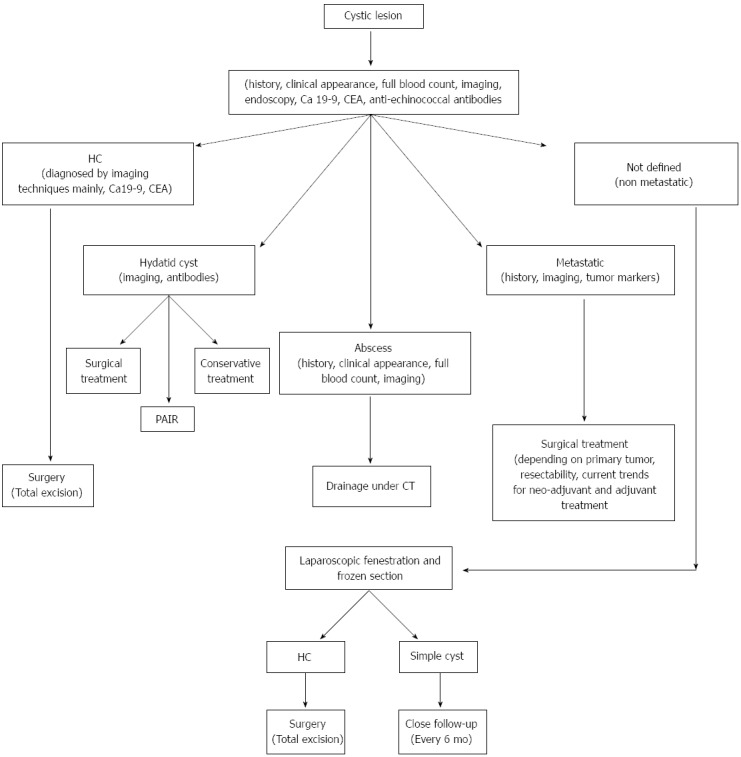
Cystic formations within the liver are a frequent finding among populations. Besides the common cystic lesions, like simple liver cysts, rare cystic liver lesions like cystadenocarcinoma should also be considered in the differential diagnosis. Thorough knowledge of each entity's nature and course are key elements to successful treatment. Detailed search in PubMed, Cochrane Database, and international published literature regarding rare cystic liver lesions was carried out. In our research are included not only primary rare lesions like cystadenoma, hydatid cyst, and polycystic liver disease, but also secondary ones like metastasis from gastrointestinal stromal tumors lesions. Up-to date knowledge regarding diagnosis and management of rare cystic liver lesions is provided. A diagnostic and therapeutic algorithm is also proposed. The need for a multidisciplinary approach by a team including radiologists and surgeons familiar with liver cystic entities, diagnostic tools, and treatment modalities is stressed. Patients with cystic liver lesions must be carefully evaluated by a multidisciplinary team, in order to receive the most appropriate treatment, since many cystic liver lesions have a malignant potential and evolution.
Keywords: Caroli; Cystadenocarcinoma; Cystadenoma; Cystic tumor; Echinococcus; Gastrointestinal stromal tumors; Hepatic lesion; Hydatid cyst; Liver cyst; Metastases; Polycystic liver disease.
Figures
References
-
- Caremani M, Vincenti A, Benci A, Sassoli S, Tacconi D. Ecographic epidemiology of non-parasitic hepatic cysts. J Clin Ultrasound. 1993;21:115–118. - PubMed
-
- Hai S, Hirohashi K, Uenishi T, Yamamoto T, Shuto T, Tanaka H, Kubo S, Tanaka S, Kinoshita H. Surgical management of cystic hepatic neoplasms. J Gastroenterol. 2003;38:759–764. - PubMed
-
- Vogt DP, Henderson JM, Chmielewski E. Cystadenoma and cystadenocarcinoma of the liver: a single center experience. J Am Coll Surg. 2005;200:727–733. - PubMed
-
- Carson JG, Huerta S, Butler JA. Hepatobiliary cystadenoma: a case report and a review of the literature. Curr Surg. 2006;63:285–289. - PubMed
-
- Ishak KG, Willis GW, Cummins SD, Bullock AA. Biliary cystadenoma and cystadenocarcinoma: report of 14 cases and review of the literature. Cancer. 1977;39:322–338. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
